

Healthcare in 2026: Still Faxing, Already Talking About AI
TL;DR: Three stories from a single day highlight a familiar pattern in healthcare technology: a pharmacy text message with the wrong hours that nobody has fixed, medical imaging that has to be mailed on a physical CD in 2026, and health systems exploring AI while still relying on fax machines. The common thread isn't bad technology — it's the gap between knowing something should be better and actually making it better.
I had one of those days recently where healthcare technology seemed determined to remind me how far we still have to go.
Three separate experiences, all in the same day, each raising a version of the same question: why don't things get fixed? Some of these problems are genuinely hard — getting different health IT systems to talk to each other is no small thing. But that makes it even more puzzling when the easy fixes don't happen either.
A Prescription Sent to the Wrong Pharmacy
My wife broke her ankle about six months ago. As part of her continued recovery and follow-up care, her surgeon prescribed an antibiotic — and the prescription was sent to the hospital's outpatient pharmacy, about 30 minutes from our home, instead of her preferred CVS down the street. Oops. A mistake.
That kind of thing happens. What made the errand more interesting was the conflicting information about when the pharmacy actually opened.
The text message my wife received said the pharmacy was open from 9 AM to 5 PM. But she remembered calling previously and hearing an automated voice message that said 7:30 AM. I called and heard the same thing. I couldn't get through to a human to confirm, so I decided to take my chances and show up at 7:45, since that worked better for my schedule.
They were open. I got the prescription quickly. No delay. No drama.
But I mentioned to the pharmacy tech — politely — that the text message said 9 AM while the phone system said 7:30. M
y wife and I had been talking about this the night before, and I'd even mentioned it earlier that day to some healthcare executives I was speaking with. We all agreed there was at least a 50% chance the reaction would be something like, “Yeah, we've brought that up and it hasn't been fixed.”
The pharmacy tech kind of smiled and half-rolled his eyes — not at me, but at the situation.
He said, almost word for word:
“Yeah, we've been trying to get marketing to fix that for a year.”
The problem had been known. For a long time. But not fixed.
The Futility Factor, in a Pharmacy
I wasn't surprised. But it's still striking every time you hear it.
This is what Ethan Burris, a researcher at the University of Texas, calls the “futility factor.” His research shows that one of the top reasons people stop speaking up at work isn't fear of punishment. It's the belief that speaking up won't lead to anything changing.
People shift from “I'm afraid to speak up” to “It's just not worth the effort.”
That pharmacy tech had clearly raised it before. I'm guessing he didn't get punished for that. There probably wasn't a “fear factor” involved.
But after a year of nothing happening, you could see the resignation. They'd done their part. The system hadn't responded.
Now, in this particular case, the mismatch probably creates more confusion than harm. Having the pharmacy open earlier than expected is better than the reverse — imagine showing up at 7:30 only to learn it doesn't open until 9.
But the question still matters: why doesn't a seemingly simple fix in a text messaging system get done?
Is it perpetually seen as a low priority by the people who control that system? Is it lost in a queue between marketing and IT? Or is it something more cultural — where the response to the suggestion was essentially, “That's not really a problem”?
Whatever the reason, the pharmacy staff is stuck living with the disconnect. And after enough time, most people stop bringing it up. Except for the patients who experience the problem for the first time.
Medical Imaging in the Age of Physical Media
Later that same day, I had my own appointment at an spine clinic — dealing with some numbness in my left foot that seems to be caused by a nerve impingement.
I'd had an MRI done in December at a standalone imaging center in Texas during the holidays. (You know the drill — get the expense in before the deductible resets in January.)
The PA treating me asked if I had the physical disc with the report and images. She hadn't seen either yet.
It might have helped if the office had asked me to bring it in advance. Or maybe I should have assumed they'd need it. But not every patient knows that.
Here's the part that gets interesting.
As the patient, I had access to the report and imaging through the imaging company's patient portal. And because this was healthcare, and I expected to wait, I had my laptop with me — and sure enough, the appointment was about 30 minutes behind schedule.
I had received an email in January that said, “You've Got Images!” When I read that to her outloud when I found it, the PA and I are of the age where we kind of simultaneously made the AOL “You've Got Mail” joke.
I logged in, she took the laptop, and got what she needed. That worked fine in the moment.
But for the clinic's records, she still needed me to call the imaging company and request that they mail a physical CD with the report and images.
Let me say that again: in 2026, the process for transferring digital medical images from one provider to another involved mailing a physical disc, which would then presumably be re-digitized into the clinic's system.
I asked the PA why it wasn't possible for the imaging center to send her a login. She said they couldn't access a system like that… because of HIPAA.
I'm not a HIPAA attorney, but that seems like a situation where the regulation — or more likely, the interpretation of the regulation — is getting in the way of something that should be straightforward. If I'm the patient and I want my orthopedic PA to see my imaging, I should be able to click a “share” button and grant access. That technology exists in virtually every other context.
In the American Airlines website or app, I can click a quick “Share” button to send my itinerary and even all of my reservation codes to somebody else of my choosing.
I've been in a similar situation before where an organization had to send a FAX to request high-tech digital CT imaging, which was then sent to them on a physical disc. In 2026.
It's not a HIPAA violation for me to share one of my own images here:
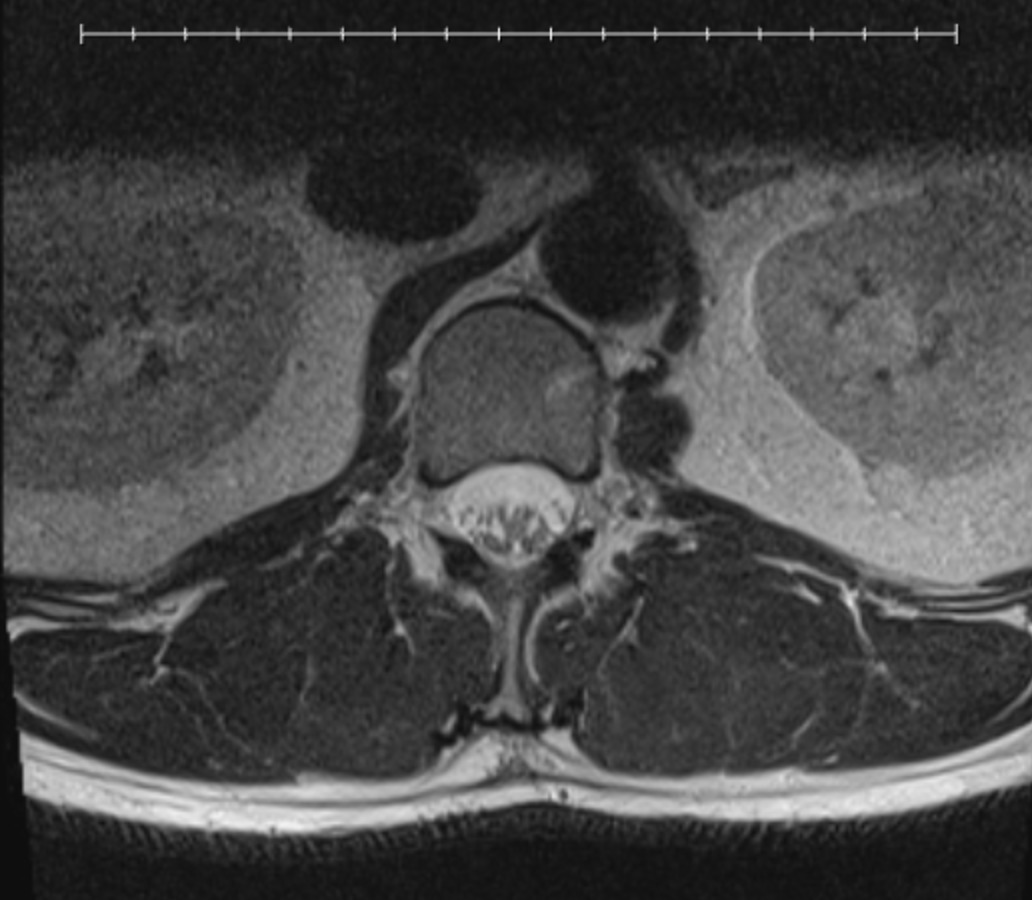
The PA was good at navigating the system to find the image that shows the one disc that's degenerated severely compared to the others that look normal. I wasn't able to find that image, which is the one I wanted to share.
I don't know exactly what we're looking at but we're looking at a horizontal slice of my body with the spinal column there. I think.
Maybe AI Can Help Us Eliminate the Fax Machine
That brings me to the third moment from this day.
Earlier, in my conversation with the healthcare executives, the topic of AI came up. They were asking about the possibilities for incorporating AI into their organization's “quality system” — which was their way of describing their Lean management approach.
It's a great question, and one a lot of organizations are wrestling with right now.
But we all had a good laugh at my observation about the juxtaposition: here we are in 2026, and health systems are simultaneously using fax machines and mailing physical CDs… while also experimenting with cutting-edge artificial intelligence.
Maybe we need to harness the power of AI to figure out how to stop faxing and mailing CDs.
The Real Question
These three stories are different in scale. One is a text message with the wrong hours. Another is a nonsensical process for sharing medical images. The third is a philosophical question about where to invest in new technology when old problems remain unsolved.
But in each case, the people closest to the work already know something isn't right. The problem isn't awareness. It's the gap between seeing the problem and having the ability — or the authority — to do something about it.
Sometimes the people who control the system don't experience the pain, so fixes stay at the bottom of the list. Sometimes systems weren't designed to talk to each other, and nobody owns the gap. Sometimes the suggestion just gets shrugged off as “not a real problem.”
And sometimes, as Ethan Burris's research reminds us, people simply stop asking. Not because they're afraid. Because they've learned it won't matter.
That last one is the quietest failure mode — and maybe the most costly. The problems don't go away. People just stop pointing them out.
Question for Discussion:
Where are the “we've been trying to get that fixed for a year” problems in your organization — and what's actually standing in the way?






