

Before “Just Culture,” There Was NUMMI: Learning Instead of Blaming
TL;DR: NUMMI proved in the 1980s what healthcare is still learning today: you can't punish your way to safety. Real improvement comes from mutual trust, system thinking, and leaders who respond to problems with curiosity–not blame.
When we talk about “Just Culture” in healthcare or psychological safety in high-reliability organizations, it's easy to view these as modern concepts. But forty years ago, on an assembly line in Fremont, California, the same ideas were already being practiced.
I found the document that tells that story–the NUMMI Management Practices: Executive Summary–in the Don Ephlin Papers at the Walter P. Reuther Library at Wayne State University in Detroit. Ephlin, a visionary UAW leader and later an MIT professor of mine, kept it because he saw something bigger in NUMMI: a model of learning, trust, and shared responsibility that could redefine labor-management relationships. Read previous posts on this report.
Here's the cover of that report.

As I've explored in Lean Hospitals and The Mistakes That Make Us: Cultivating a Culture of Learning and Innovation, the best systems for safety and improvement are those that treat people as partners in problem-solving. The NUMMI story captures that same truth decades earlier–and shows what happens when psychological safety becomes part of daily work, not a corporate program.
This short but powerful document isn't just about car manufacturing. It's about how people learn, lead, and work together when the goal isn't control–it's continuous improvement through respect.

The Shift: From Blaming People to Improving Systems
Long before the term Just Culture existed, NUMMI's leadership understood something Dr. W. Edwards Deming had been preaching for years: most problems come from systems, not individuals.
The Executive Summary made that explicit:
“When a problem occurs, the emphasis is on finding and eliminating the cause rather than finding someone to blame.”
That single sentence reflected a fundamentally different management mindset. It reframed management's role–from judge to investigator, from disciplinarian to coach.
Healthcare's Just Culture movement would later make the same case: if you want safety, you can't lead through fear. You must build systems that help prevent systemic mistakes and human error. And create a workplace where it's safe to learn from mistakes.
Stop the Line: The Power of the Andon Cord
NUMMI didn't just talk about empowerment–it designed for it. Every team member on the assembly line had the authority to pull the andon cord when something went wrong.
“Each employee is responsible for the quality of his or her work and has the authority to stop the line if a problem cannot be corrected immediately.”
In most American factories of the time, stopping the line was unthinkable–a punishable offense. At NUMMI, it was a sign of pride. The message was simple: protecting quality is everyone's job.
In healthcare today, that's the equivalent of a nurse speaking up during a procedure or a resident pausing a medication order. Both are acts of respect for safety–and both depend on systems that encourage people to speak, not silence them.
American factories, like my GM engine plant in 1995, told workers to have pride and that quality was their job. But the workers weren't empowered to do what was necessary to ensure quality. Bad decisions by management actively hamstrung their efforts to do the best job possible for the customer–for example, leaders putting quantity before quality.
Read more: 20+ Years Ago at GM: The Quality Death Spiral of Bad Management & Blaming Workers
Problem Solving as Learning
NUMMI turned problem-solving into a shared act of learning, not a hunt for blame.
“Supervisors are trained to help employees solve problems at the source, not to assign fault.”
and
“NUMMI's problem-solving process focuses on why the problem occurred, not who made the mistake.”
Those sentences could appear word-for-word in a hospital safety manual today. In both settings, the principle is the same: improvement comes from asking why, not who.
Read more: Why “Who?” Is the Worst Root Cause Question: A Lean Lesson From Owls
NUMMI leaders didn't demand immediate perfection–they wanted learning cycles. Every problem became an opportunity to strengthen the system, not to shame the person–an idea that echoes what I call “a culture of learning” in The Mistakes That Make Us.
Poka-Yoke: Designing for Humanity
While the document doesn't use the Japanese term poka-yoke (error-proofing or mistake-proofing), it describes it perfectly:
“The work system is designed to prevent errors whenever possible, and to detect and correct them immediately when they occur.”
NUMMI recognized that humans make mistakes because they're human–and that systems should anticipate that.
In healthcare, we call this safety by design: barcode medication checks, pre-surgery timeouts, and forcing functions that make the right way the easy way. The principle is the same–don't blame people; design systems that protect patients and staff.
Trust as the Root of Safety
What made NUMMI work wasn't just its processes–it was its culture. The Executive Summary opens with the foundation of it all:
“The NUMMI philosophy is based on mutual trust and respect between management and employees, a shared responsibility for quality, and the belief that problems are best solved by those who do the work.”
That's psychological safety, decades before Amy Edmondson made the term popular in business.
At NUMMI, speaking up wasn't defiance–it was duty. Team members, union representatives, and managers worked from a shared understanding: we solve problems together, not alone.
That's the same cultural leap healthcare organizations still struggle to make today. The question is not if people will err–it's whether the system makes it safe for them to admit it and learn.
Trust That Delivered Results
This mindset wasn't just ethical–it was effective. NUMMI showed that respect for people was not only possible, but economically effective.
Within a year of opening, the same Fremont workforce that had once been called “the worst in GM” was matching–and soon exceeding–the productivity and quality of Toyota's own plants in Japan. Absenteeism, which had been around 20% under old management, dropped below 3%. Defect rates plummeted.
Managers later credited this system of mutual trust, open problem-solving, and no-blame learning–what we'd now call leadership standard work–as the catalyst for breakthrough performance. When employees could stop the line, surface problems, and fix them at the source, quality became built in, not inspected in after the fact.
The Executive Summary captured this cause-and-effect clearly:
“Quality, productivity, and morale are the natural results of a system in which problems are seen as opportunities for improvement rather than as failures.”
NUMMI's success sent shockwaves through the industry. It demonstrated that a plant's performance was a mirror of its management philosophy — and that psychological safety was a competitive advantage long before anyone called it that.
“If that was true on an assembly line, imagine what it could mean in a hospital, a clinic, or any organization built on human skill and teamwork.”
Why GM Didn't Learn Broadly Enough from NUMMI
As extraordinary as NUMMI's success was, the real tragedy is how little of it spread within General Motors.
NUMMI had demonstrated beyond question that American workers could thrive under a system of respect, teamwork, and continuous improvement. Yet GM largely treated it as an anomaly–a joint venture to be studied, not a model to be scaled.
Inside the company, old mental models proved hard to shake. Command-and-control habits, fear of union backlash, and internal politics all conspired against learning. The NUMMI Management Practices Executive Summary itself was marked “GM Confidential”–a symbol of how the lessons were contained when they should have been shared.
Toyota made learning a daily discipline; at GM, it too often became something assigned to a department. The difference was everything.
In my 2015 post about This American Life's NUMMI episode, I reflected on this same dynamic: “GM did learn many lessons, but not enough to save the company.” It wasn't for lack of knowledge–it was a failure of leadership humility and organizational will.
The Fremont experiment had proven that quality, productivity, and morale could coexist. But too often, GM's broader culture reverted to managing by compliance, not curiosity. It took decades–and bankruptcy–for that lesson to truly sink in.
The cautionary takeaway still applies far beyond manufacturing: a single island of excellence can't transform an organization that isn't ready to learn.
I saw echoes of this firsthand a decade later inside GM— pockets of Lean thinking surrounded by layers of bureaucracy still clinging to the old management playbook.
Read more: Throwback Thursday: “This American Life” on NUMMI Lessons, “Labor Notes” Still Hates Lean
Healthcare's NUMMI Opportunity
Healthcare faces a similar challenge today. We have our own “NUMMIs”–pockets of excellence where leaders replace blame with learning–but the question remains: how fast, and how broadly, can those lessons spread?
Today, a growing number of hospitals are rediscovering the same truth NUMMI proved in the 1980s:
You can't punish your way to safety.
Healthcare's “andon cords” aren't literally hanging above every patient bed. They are incident reporting systems. Our poka-yoke devices are barcoding scanners and electronic medication checks. Our team leaders are charge nurses, residents, and attending physicians who must guide, not intimidate.
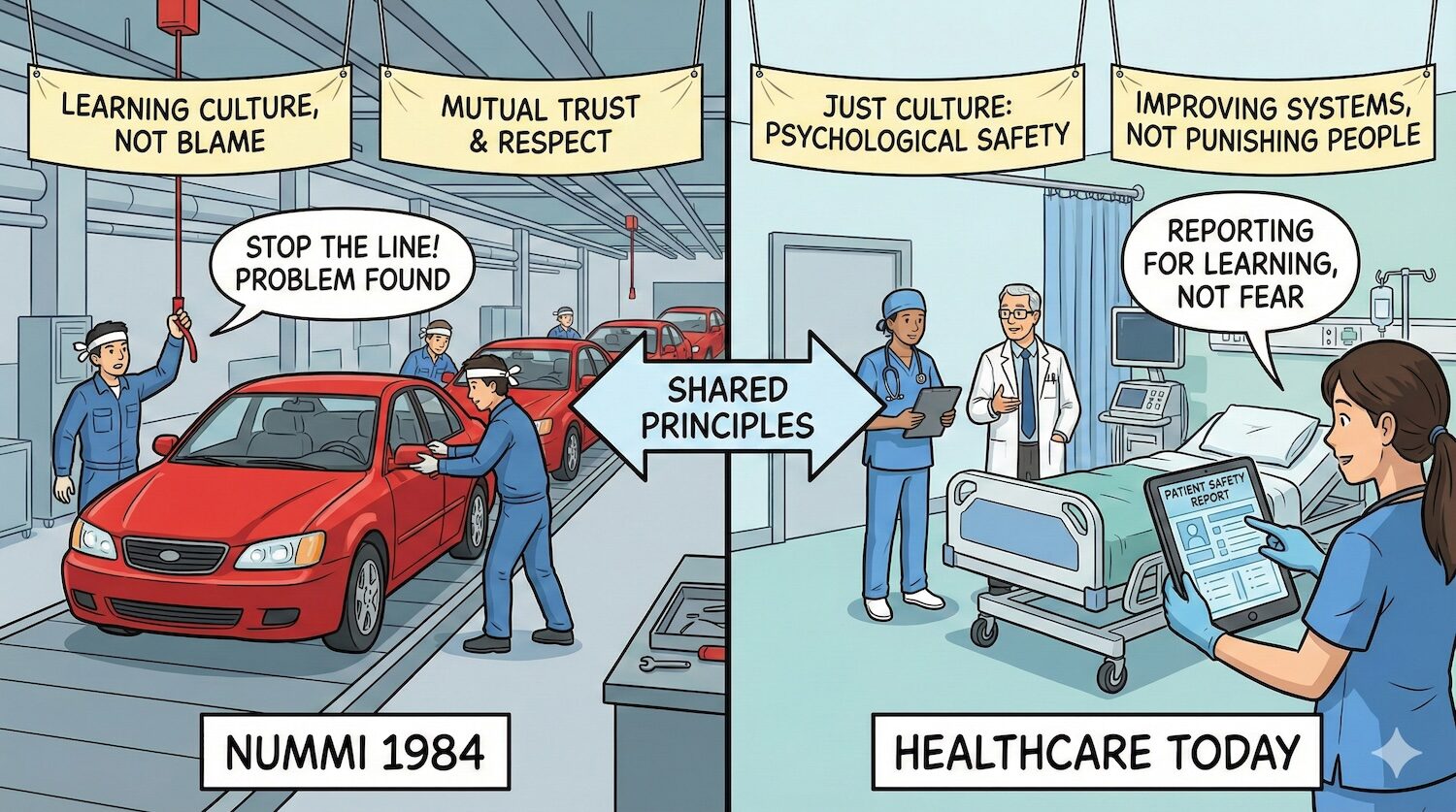
And our shared challenge–just like NUMMI's–is how leaders respond when something goes wrong. Do we look for someone to blame, or do we look for something to learn?
The illustration below shows how it should be in healthcare. It's, sadly, not the norm today.
Read more: You Can't Punish Your Way to Perfection: Why Blame Fails and Learning Works
The Leadership Lesson We Still Haven't Fully Learned
When the line stopped at NUMMI, no one panicked or pointed fingers. They investigated, learned, and improved.
Imagine if every time a near miss occurred in healthcare, leaders responded the same way–not with shame or silence, but with curiosity and collaboration. That's how safety evolves–from compliance to compassion, from fear to learning.
As the NUMMI summary put it, simply and powerfully:
“When a problem occurs, the emphasis is on finding and eliminating the cause rather than finding someone to blame.”
That's not just Lean–it's leadership.
These lessons aren't frozen in history. They continue in every organization that learns instead of blames. Whether it's a hospital adopting Lean thinking, a tech team experimenting safely, or a factory empowering its people to improve every day–the spirit of NUMMI lives on. That's the same spirit I've tried to capture in Lean Hospitals and The Mistakes That Make Us: that better systems–and better leaders–start with respect and learning.
And thanks to Don Ephlin and the Reuther Library archives, we have the privilege of rediscovering this truth: long before anyone called it “Just Culture,” NUMMI was already showing us what it looks like to lead with trust, learning, and respect for people.







While reading this blog post I found it very interesting how NUMMI is explained. The author discusses that NUMMI results in operational performance because of leadership mindsets and system designs. Most people might view punishment or very strict work environments as a way to discipline and teach employees, but this is incorrect. This article explains that viewing problems as learning opportunities rather than failures is much more beneficial. Additionally, this connects to identifying the root cause of problems and how to continuously improve them. I also believe that creating an open minded and safe environment for employees to speak their mind promotes growth, especially fixing daily issues that only employees might experience. Overall, I agree and enjoyed reading this article because it explains how trust and respect from leadership and promotes employees to speak up and identify issues at the cause.