


TL;DR: After three editions of Lean Hospitals, I am not planning further updates to the book. This post reflects on how the opening of Chapter 1 has evolved since 2008, including John Toussaint's second-edition foreword, and shares a revised “Need for Lean” introduction written for the realities hospitals face in 2026.
After three editions, Lean Hospitals has reached a natural stopping point for me. I've known that for a while. Some people ask, “Are you doing to write a 4th edition?” The answer is no, but I did propose a version as an April Fool's Joke a few years back.
The first edition was published in 2008, and the third edition came out in 2018. For a number of reasons, I am not planning any further updates to the book. That does not mean Lean is over, or that the problems are solved. It simply means my work with the publisher on this book has run its course.
Even so, I recently felt an urge to revisit the very beginning of Chapter 1.
This reflection was an opportunity to think again about how I would describe the need for Lean in hospitals today, given what has changed — and what has not — since 2008.
How the Book Originally Began
When the first edition was published in 2008, Chapter 1 opened with a simple statement:
“Many hospitals are struggling.”
That was true then, and it is still true in 2026. A bit negative, but true–and accepted.
The first page:
BTW, do you see the spelling error (that wasn't my fault)? You can get the full first chapter here.
For the second edition, the foreword by John Toussaint, MD, began with a much more direct declaration:
“America is broke.”
John went on to argue that healthcare leaders had caused, or at least contributed to, this reality by failing to focus on delivering high-value healthcare. He defined value plainly as quality divided by cost, and he argued that poor quality combined with high cost results in poor value. His framing was intentionally provocative, and for many readers, it resonated.
The healthcare value conundrum (or problem) is certainly not just an American problem:
Looking back, what stands out to me is not that either opening was wrong. If anything, they have both aged uncomfortably well.
What feels different now is not the existence of struggle, but its persistence and normalization. It seems too many accept that the system is broken, but not fixable.
So I tried a reflective exercise. I rewrote the opening of Chapter 1 as if I were writing it for the first time today, informed by nearly two decades of working in healthcare since the book was first published.
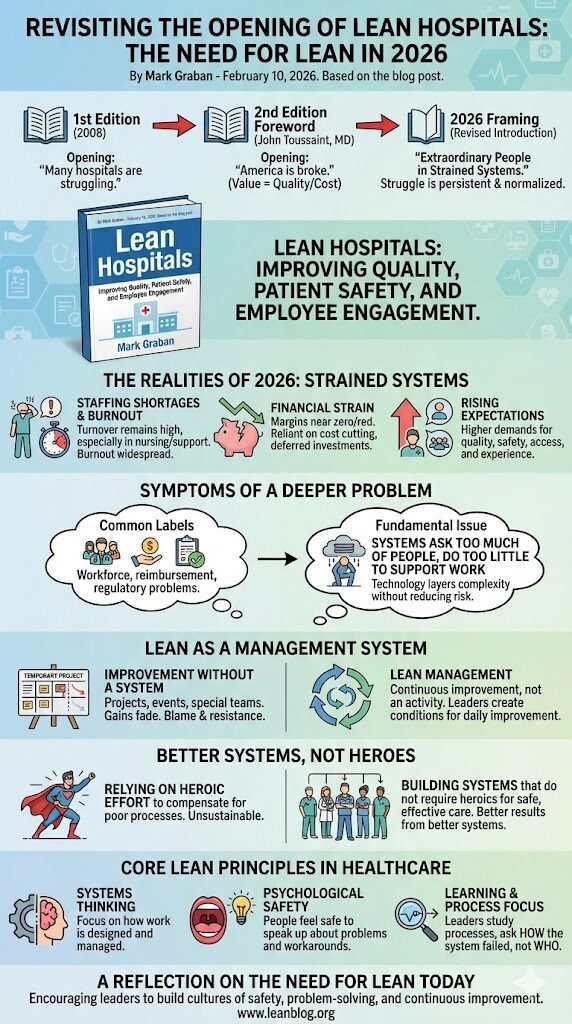
The Need for Lean in 2026
Extraordinary People in Strained Systems
Healthcare professionals do extraordinary work every day, within systems that too often make that work harder, less reliable, and more exhausting than it needs to be.
Many of the challenges hospitals face no longer feel temporary or cyclical. Staffing shortages persist despite aggressive recruiting and compensation efforts. Surveys continue to show that roughly half of physicians and nurses report symptoms of burnout. Turnover has slowed in some areas, but it remains well above pre-pandemic levels, particularly in nursing, pharmacy, and support roles.
Financial pressure adds to that strain. Many hospitals operate with margins near zero or in the red. Even organizations that appear stable often rely on cost cutting, deferred investments, or one-time fixes to remain viable. At the same time, expectations for quality, safety, access, and experience continue to rise.
Taken together, these conditions are difficult to dismiss as isolated or short-lived.
Symptoms of a Deeper Problem
These challenges are often described as workforce, reimbursement, or regulatory problems. Each of those labels captures something real.
Together, they point to something more fundamental.
They point to systems that ask too much of people while doing too little to support the work itself. That is not a problem individual clinicians or staff can solve on their own. It is a problem that must be addressed by leaders and staff working together within the health system.
For years, improvement efforts in healthcare have focused on asking people to work harder, adding policies, implementing technology, or launching the next breakthrough initiative. Electronic health records, analytics platforms, and automation have delivered real benefits. They have also added complexity, documentation, alerts, and workarounds.
Too often, new tools are layered on top of broken processes, increasing cognitive load without meaningfully reducing risk.
When improvement occurs, it is frequently separated from daily work.
Improvement Without a System
Lean remains necessary today not because healthcare has failed to improve, but because improvement has too often been treated as an activity rather than as a management system.
In many organizations, improvement still happens primarily through projects, events, or special teams. Leaders sponsor it. Experts facilitate it. Frontline staff participate when time allows.
When gains fade, the explanation is familiar. Lean did not stick. People resisted change. Healthcare is simply too different or too complex.
A more useful conclusion is that the system was never designed to support continuous improvement in the first place.
Systems, Not People, Create Most Problems
The most serious problems facing healthcare today — patient harm, delays, rework, moral distress, turnover, and financial strain — are largely the result of how work is designed and managed. They are not caused by a lack of effort, caring, or professionalism.
In fact, healthcare often depends on extraordinary effort from clinicians and staff to compensate for poor processes.
That dependence is not sustainable.
As Kim Barnas and John Toussaint have suggested, healthcare needs to move beyond heroes. Not by lowering expectations, but by building systems that do not require heroics to deliver safe, effective care.
Lean offers a different premise. Better results come from better systems, and the people doing the work are best positioned to improve those systems when leaders create the right conditions.
Lean as a Management System
This is not about copying manufacturing or pursuing efficiency for its own sake. It is about adopting a management approach that makes problems visible, recognizes variation, and encourages learning rather than blame.
In healthcare, psychological safety is not an abstract cultural aspiration. When people feel safe to speak up about problems, near misses, and workarounds, leaders gain a more accurate picture of reality. When they do not, that picture is incomplete.
When leaders respond to bad news with pressure or blame, they unintentionally teach the organization to hide problems rather than solve them. Over time, the gap between what leaders believe is happening and what patients and staff experience grows wider.
Lean helps close that gap by changing how leaders think and behave.
Instead of asking who made a mistake, Lean encourages leaders to ask how the system made the outcome likely. Instead of reacting to metrics, leaders study processes. Instead of relying on inspection and compliance, they focus on building capability and learning at every level of the organization.
Setting the Stage for Lean Principles
The need for Lean in 2026 is not primarily about doing more with less. It is about creating healthcare organizations that can learn faster than the problems they face, including the problems that have not yet fully emerged.
To understand how Lean addresses these challenges, it is important to be clear about what Lean is and what it is not. Lean is often misunderstood as a set of tools or cost-cutting techniques. In reality, Lean is a management system grounded in respect for people and a deep focus on how work actually gets done.
The sections that follow introduce the core principles of Lean as they apply to healthcare. They emphasize systems thinking, learning from problems, and leadership behaviors that enable improvement to occur every day, not just during special initiatives. The examples that follow show how organizations move from relying on heroic effort to building systems that consistently support safe, effective care.
A Reflection, Not a New Edition
I am not publishing this as a new edition, and I am not suggesting that the book is suddenly outdated or wrong. If anything, the core ideas have held up better than I might have expected.
This was simply an opportunity to reflect on how I would explain the need for Lean in hospitals today, knowing what I know now.
I am curious what stands out to you.
- Does this 2026 framing resonate more than the earlier openings?
- Does it feel more accurate for the reality hospitals face today?
- Or does the earlier, more blunt language still feel necessary?
I do not have a firm conclusion here. Just an observation, and a question worth thinking about. What do you say?






{kind=link}