

Today is the first day of the 5th annual Lean Healthcare Transformation Summit. Follow along on Twitter with hashtag #HCSummit14 to see my tweets and thoughts from others. I will be adding updates to this post during the day, as well. These are not meant to be complete notes or a transcript… but quotable and interesting thoughts or comments from each talk.
Getting Started
We have about 40 CEOs in attendance in a crowd of about 600+. Significantly more than past years and that's a very good sign, I think.
Who is here?
- 600 attendees from 277 organizations
- 43 U.S. states, 4 Canadian provinces, and 5 countries represented
Paul O'Neill
(via video, following up last year's talk)
Habitual excellence and safety is a moving target… not resting on any laurels.
Healthcare is the most dangerous industry in the US in terms of OSHA recordables… goal should be an injury-free workplace.
Do you even know the data for your hospital? How many injuries occur? Ae you happy with that? Do you learn from every thing that goes wrong?
Cincinnati Children's Hospital has focused on employee safety and rate has fallen by more than half, and they used to be “average” compared to children's hospitals. If you pay attention every day and truly care about your people, you can approach an injury-free workplace.
Stand if you know your real-time injury rate… very few people actually stood up.
Helen Zak
The ideal state is everybody involved in solving problems every day… to improve things and to provide the best patient care.
John Toussaint, MD Keynote
The major problem in healthcare: at least 210,000 deaths per year associated with preventable harm in hospitals. This is the problem we need to solve.
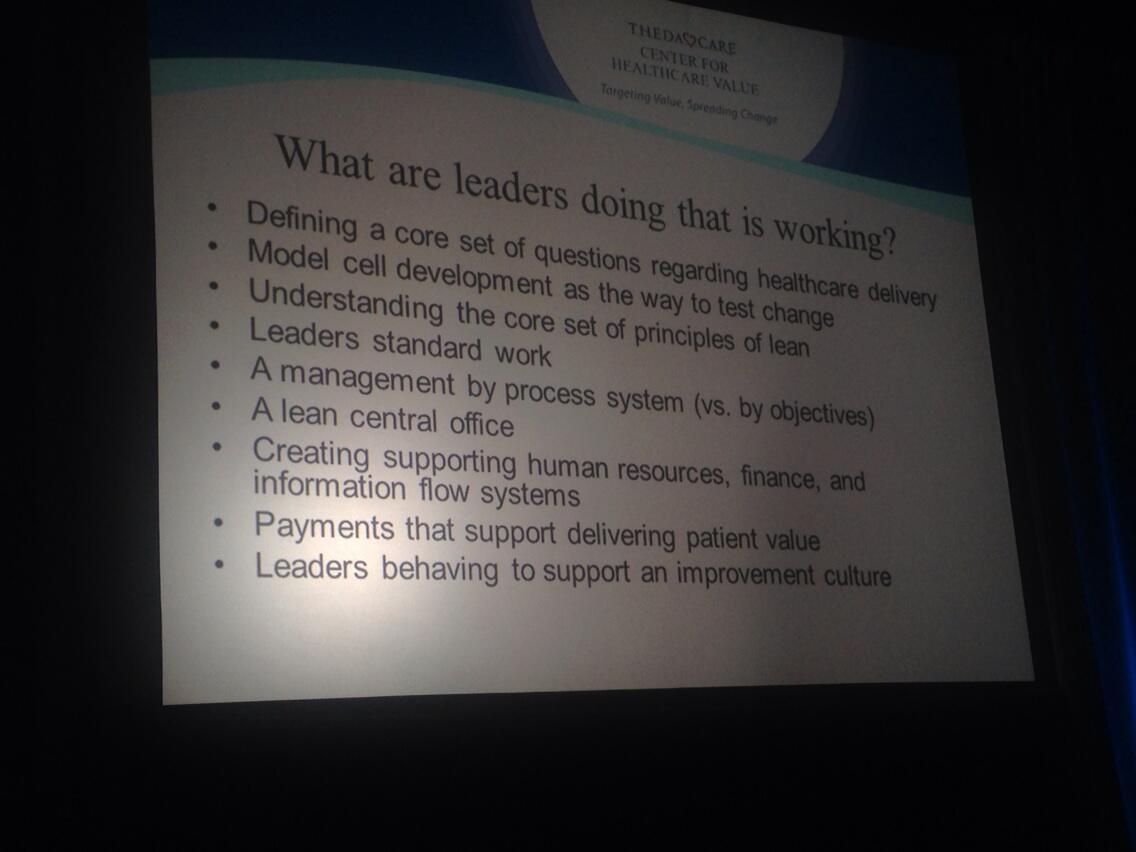
We're find a core set of ideas out there that are actually working… I'm getting pretty excited about that. What are they doing? (Picture via Twitter).
Start with an important problem that matters (like patient safety).
The story John told last year about his mother in law almost dying from errors (she's doing fine now).
John shared video and data from his own primary care appointment as a patient. Lab specimen collected and resulted within just 14 minutes (done on sight). Data is available for the doctor and patient during the appointment. John can see data in his own personal medical record chart online (data and trends over time).
Our traditional top-down command-and-control management system has got to go out the door if we're going to change… to deliver better value (higher quality and lower cost).
When I was CEO, I was “thrilled we had 33 brilliant strategies” that had no bearing on people's daily work. Now ThedaCare has four “breakthrough objectives” and focus: People, Safety, Shared Growth, Productivity. Using A3 thinking to take these strategies out for discussion and creating alignment with the front line. “What really is the problem and how do these strategies help?”
“Most of what we call management consists of making it difficult for people to get their work done.” (Peter Drucker)
“Why we never listened to Dr. Deming, I don't know. That must change. We are delivering unreliable care.”
John shows a video of a manager talking with a team about the orders getting onto the wrong patient chart (error). It had happened before. Manager leads by asking questions. “How do we prevent this from EVER happening again?” Staff figured it out. Nurse was given TIME to go work on a new process and new standardized work to help prevent this. This is how we don't pass the defect on to the next customer. Not talking about it 60 days later in some “quality meeting.” The only chance to fix the problem is when it happens. That's missing in healthcare. That's what we need to create.
A “no layoff philosophy is very very important.” If you layoff people as a result of Lean improvements, good luck getting people to participate in the future. We've guaranteed people that they're going to have a job (it might change).
We need ongoing performance management discussions with people, not just an annual review.
“We're spending too much money on software that delivers no value.” We need to stop buying stuff and actually utilize what we have. Using data as actual “business intelligence.”
Can we get rid of the traditional budgeting process? All of this budgeting work doesn't really reduce costs. Look at “Beyond Budgeting” principles. ThedaCare eliminated and redeployed, 20,000 hours of budgeting time.
“Lean is NOT a cost reduction methodology.”
Patrick Conway, MD Keynote
Bio — Deputy Administrator for Innovation & Quality CMS Chief Medical Officer (still works as a pediatrician)
It seems accurate to describe Lean healthcare as “a movement.”
Current state of healthcare: producer-centered, volume driven, fragmented, fee-for-service, and unsustainable.
Future state: people-centered, outcomes driven, sustainable, coordinated care, new payment systems and policies (value-based purchasing, ACOs, shared savings, medical homes, etc).
“It's not just cost reduction; it's reduction of waste and providing more value for patients.”
Information Technology is a means, not an ends.
We're at the lowest cost growth in Medicare per capita spending in the last 50 years.
Seeing improvements in fewer readmissions (see control chart), lower CLABSI, fewer elective pre-term births. Reductions in patient harm events. 9% reduction from 2010 to 2012 (preliminary data), estimated 15,000 lives saved, 540,000 fewer injuries, and $4 billion in cost savings.
“At the end of the day, it's front line people delivering the improvements and value to patients.”
The CMS Innovation Center: purpose is to test innovative payment and service delivery models to reduce spending while quality is same or better (ideal is better quality and lower cost).
Testing bundled payments – bundles cost of services for an episode of care with quality measures related to the episode. Allows providers to innovate, remove waste from the system, and improve quality.
Starting the “Lean culture change journey” within CMS – fairly early in the journey.
Made a commitment about two years ago to becoming a culture of continuous improvement. Hired “Lean fellows” from companies like Intel and others, mainly outside of healthcare.
Improving manager commitment and employee engagement, making this a part of daily work, aligned to strategic objectives, performance plans, and recognition. Employees see Lean as “how they'll get promoted” or it will otherwise limit their opportunities to succeed.
“Lean is a culture of continuous quality improvement made through small, incremental changes to achieve an ideal state.”
HHS Lean Team guiding principles (see picture)
There are kanban boards all over the place in CMS (“we're spending so much in post its” said a purchasing person)
They are doing a number of Kaizen Events to improve different processes.
Why is Lean working there?
Strong manager commitment at all levels, including senior leaders
Dedicated staff and space.
Incorporated into everyday work for staff and managers, recognition for involvement
Standardized tools, processes, training, and success measures
Not all leaders loved the idea of taking front-line employees off of regular work to focus on improvement.
Patient goal – Fewest number of days in the hospital, maximize he number of days at home with good health. Nobody is measuring that.
Learning Session: “Experiments Around the Network”
Cleveland Clinic – Building a culture of continuous improvement
Why work on this now? Challenges “require engaging all caregivers in improvement” — this was a new realization from the CEO and another senior medical leader.
Before: A team of continuous improvement experts would do a project. We *did* see better results, but it was reactive. The ownership of the problem and the solution was with the expert team, not those who really did the work.
Goal: Create a culture where every caregiver is empowered and expected to make improvements every day. Problem was not a lack of desire. Decided people don't have capabilities to see problems as opportunities and to fix things.
What to do: 1) build caregiver capabilities 2) capable caregivers can teach others, creating a multiplier effect
Model Area Pilot – a controlled experiment, test a hypothesis, have a visible model, demonstrate results, and enable continuous learning (PDCA). Did some awareness training that was hands on and driven to application… based on identifying opportunities and problems that they see. They confirmed capability by doing weekly report outs, looking for Lean behaviors and results. Continued to do “PDCA so ridiculously rigorously.”
Did 130 Kaizen improvements — 1 per person per month (empowered and expected). 1652 hours saved.
Can every caregiver articulate: What are you working on? Why are you working on it? How are you performing? What are you doing to improve it?
Health East – Implementing 100 Ideas a Day, Every Day
Frontline Management System: Includes measures (run charts specific to four pillars for Health East), huddles, improvement boards (visually manage ideas).
Goals: Improve processes AND develop problem solvers.
Using a visual idea board… limit of five ideas being worked on at any given time.
Generated 80 ideas in six months in six cohort teams. Wanted more improvement than that… so what to change? Simpler cards. Added metrics boards (daily performance view). Added huddles.
Planned a cohort-based rollout, would have taken three years… too slow. Adjusted the plan to be three months given the need for improvement.
How to support 300 teams… 300 improvement and measurement boards?
Varying levels of leadership understanding about what was needed to drive Kaizen.
Established a daily two-hour long no meeting zone.
Results: FY13: 76 ideas per day. FY14: 107 ideas per day
What impact did it have? Met pillar targets in all four categories and were exceptional in three of those areas.
Next steps: Progression from recognizing problems to solving problems to aligning them with strategy. Improve coaching behaviors.
Kim Barnas Keynote
Bio – her book Beyond Heroes – listen to my podcast with her
What she's describing is “OUR” management system (ThedaCare's) not “THE” management system. A system is dependent on culture and other factors. Don't copy blindly.
Call to action — there was not a consistent business management system within ThedaCare that could be taught to managers and used consistently. Goal: To develop our people to solve problems and improve performance. Do this without being a punitive environment.
Daily Stat Sheet — it's about the status of the business, today. See trends, reduce fire fighting, solve problems that could be anticipated. The stat sheet guides discussion through questions… “it's not a checklist.”
Purpose of the daily huddle — to see waste and defects and solve problems around that waste.
“We used to be a “PD” organization (Plan / Do), we weren't very good at “SA” (Study / Adjust).”
“Lean doesn't stifle creativity; it helps us innovate.”
It is important to have a process in place to escalate problems when they arise so they can be resolved quickly. Escalation process means bringing resources to the problem… compared to old approach where a patient died and the investigation team couldn't (didn't) get together for 30 days.
“We use A3 thinking in every area of the business.”
“Coaching is expected at every level of the organization.”
That no-meeting zone saved me two hours a day… and we got so much more done instead of just firefighting.
It's hard for a President to coach a nurse. Simply asking a question, when there's a big power differential, can feel like criticism to the coachee.
“I had memorized my standard work, but I still carried it with me” to set an example for other leaders.
“This is a disciplined approach and requires the rigor to stay the course, improve countermeasures and remain humble.”
What do you think? Please scroll down (or click) to post a comment. Or please share the post with your thoughts on LinkedIn – and follow me or connect with me there.
Did you like this post? Make sure you don't miss a post or podcast — Subscribe to get notified about posts via email daily or weekly.
Check out my latest book, The Mistakes That Make Us: Cultivating a Culture of Learning and Innovation:


: Systemic Issues in Outpatient Surgery")




{kind=link}
{kind=link}
Great wrap up Mark! Thanks a lot for reminding me of the summit.
Cheers from Dresden, Ralf