
Three or four months ago, in the midst of a discussion on LinkedIn about patient safety, somebody made reference to a 1966 cover story from the magazine “Look.” Look was a very popular competitor to “Life” and the “Saturday Evening Post,” so this was written for a very general public audience.
The cover tease reads:
“OUR HOSPITALS ARE KILLING US
An alarming report on conditions in many American cities”

The cover (click for a larger view) featured a photo of Jackie Kennedy (about 30 months after JFK's assassination). I'm sure that photo and story garnered more interest, even with the muckraking text about hospitals above her.
There's another interesting cover story in the issue about downsides of standardized testing in schools. In recent years, we've seen systemic cheating in a number of cities, where teachers or principals feel pressured to change the answers on students' exams to get standardized test scores up, as I've blogged about before. Alfie Kohn (listen to my podcast with him) is quoted in this 2000 article about the problem.
Problems in our education system are a shame, but not as bad as the patient safety problems that we still face 50 years later.
I can't find the “hospitals are killing us” article online, but I managed to buy a physical copy of the magazine through eBay (and you can do the same if you like).
Hear Mark read the episode (subscribe to the podcast):
Diving Into the 1966 Article
I created a PDF of the main section of the article if you'd like to download it. The magazine is defunct, so there isn't really anyone to care about the copyright.
The article begins with a story of a preventable error that led to a patient's post-operative death.
A fact-based statement seems to be “the oxygen tank was not replaced.”
Did you notice how the article, quoting a hospital's chief of surgery, blames “the nurse?” He (it was most likely a “he” in 1966) then makes the leap to criticize “nursing care” as “abysmal.”
A more modern view of healthcare quality (including the Lean or “Just Culture” approaches) would look first to systems and processes instead of blaming an individual.
Why was a nurse put in a position to remember? Why did they rely on that? We're all human, after all, which means we forget things. We get tired, busy, fatigued, and we forget.
Why wasn't there a checklist for the nurse's critical tasks? Why wasn't there an alarm on the respirator to alert people that the tank was empty? Why wasn't there a simple mechanical timer with a bell or alarm to prompt somebody to change the tank?
That problem seems preventable, but blaming and firing “bad apples” doesn't seem to be the way to prevent errors and harm. There's still too much “naming, blaming, and shaming” in recent years, including one example of a blaming CEO that I blogged about:
And I also wrote this 2014 post about the ineffectiveness of firing the “bad apples”:
The Look article explains the “tarnished side” of medicine that is “apparently well-known to knowledgable medical critics, but has been hidden from public view.” Patients only learn “through hazardous experiences what veteran physicians are well aware of: that the hospital is a complex entity with failings that threaten quality medical care.”
Hospitals have only gotten more complex in the last 50 years. Have they gotten safer? Yes and no.
The “dangerous deficiencies” cited by the Look article are:
- medication errors
- anesthesia incompetence
- hospital-bred infection
- faulty diagnostic work-up
- blood-transfusion errors
- unnecessary or poor surgery
- inadequate nursing care
- inappropriate therapy (including unnecessary C-sections, a problem that's still being worked on today)
- negligence
It's often said that anesthesia and blood transfusions have become MUCH safer over the past 50 years. That's not because of better people, it's better process, error proofing, and technology that have led to better care in those areas, which are held up as positive examples of some parts of healthcare “getting it” and making significant improvements.
Anesthesia error death rates in the 1966 article were estimated to be one in 1,000 or one in every 2,000 cases (meaning between 9,000 and 33,000 deaths a year). This study suggests anesthesia error deaths fell to just 34 deaths per year in 2005. If anyone has better numbers on any of these areas, please post a comment below.
One thing that's still a problem today is the existence of wide ranges of estimates for numbers related to patient harm and death. The current U.S. estimates range from 44,000 to 440,000 deaths a year due to medical error. That's a huge range, right??? The lack of transparency over medical error leads to studies being done on a small number of patient records that then get extrapolated. Healthcare organizations aren't transparent, but then they complain about the estimates being inaccurate. Can they have it both ways??
Not reporting anesthesia error deaths was a really big problem in 1966:
“Death certificates, for example, severely understate the anesthesia problem. In assigning the cause of death on a death certificate, anesthesia was rarely entered…”
You probably won't see “medical error” listed as a cause of death in 2017, either.
Everything else in that bullet list of errors sounds very current. These are problems that have not been solved. The lack of transparency around errors and harm makes it impossible to compare 1966 data to, say, 2016, data. Major patient safety problems remain and I don't mean “we're not perfect.” We're still far from perfect in many ways.
The article says, “it is essential that this raging private medical dialogue about the state of our hospitals be made considerably more public.“
I would say the same in 2017.
I call the “patient safety crisis” the crisis that nobody talks about. When we see articles about process problems on the front page of USA Today, it seems like the general public reacts as if those problems are isolated, as if those hospitals are outliers. The patient safety problem is still very widespread.
The author of the piece cites medical research studies that were done in New York (the “Trussell Reports”) that were “forceful rebuttals of the mythology of the uniformly competent American hospital.”
Again, I'll point out that patient safety is a global problem (see the stats).
One of the Trussell Reports suggested that “errors in judgement or technique” in anesthesia or surgery “contribute close to 50 percent of the mortality in the operating room.” Yikes.
One study in the 1966 article suggested that of 21 “surgical deaths of infants and children” that they examined, “90 percent were the result of doctor error” and in the cases of “17 geriatric patients who died, errors were committed in the surgical care of seven of the 17.” That's 41%.
Hospital-Acquired Infections
Today, as in 1966, patients and visitors assume hospitals are cleaner and more sterile than they really are.
The article estimates that, in 1966, “well over” one million Americans contracted infections in the hospital (750,000 of those being hospital-acquired surgical infections).
Current CDC statistics say there were about 722,000 hospital-acquired infections (HAIs) in American hospitals in 2011.
Considering the U.S. population grew from 196 million to 311 million from 1966 to 2011, at least the per capita rate dropped. But HAIs are still a huge problem.
As we saw in the recent USA Today article I blogged about, the 1966 article says:
“Hospital infections are invariably a result of loose hospital standards and procedures.”
We also saw loose procedures mentioned in this recent post about Toyota helping a children's hospital reduce infections.
That's a familiar 2017 problem. Again, it's not “bad apples.” Why are hospital standards and procedures “loose?” That can be the result of understaffing / overwork, a lack of supervision, training issues, equipment and supply problems, etc.
The article discusses the wide variation in surgical infection rates at different hospitals in that era, ranging from 3 percent to 11.7 percent across five university medical centers that were studied.
What are surgical infection rates at your local hospitals? Today, you can perhaps find data on the CMS Hospital Compare site.
The article talks about a 1966 problem that doesn't exist anymore. Surgeons wore “rubber” gloves, but two doctors claimed “breaks” in “approximately 30% of gloves worn.” It sounds like “sterile disposable gloves” were a relatively new innovation, but some hospitals at the time were “attempting to reprocess them in a misguided effort to save money.”
Hospitals today have their own misguided efforts to save money (such as laying off their internal Lean / process improvement teams, as I've heard about twice already this week).
Medication Errors
The article claims that, at the time:
That blue box text seems to again blame the nurses for being the sole cause of errors, instead of looking at systems and processes.
This 2004 study at a Texas hospital found the error rate was about one in ten.
The 1966 article gives an example of a patient given distilled water intravenously instead of glucose, which caused irreversible heart damage. Another patient was mistakenly given penicillin even though their chart said “ALLERGIC TO PEN.” That patient died.
“In one reputable Florida hospital alone, they unearthed an annually projected 51,200 medical blunders!”
But when asked, a nurse was asked to recall any medication errors she had ever made and “answered confidently:”
“None – to my knowledge, I have never made one.”
This very same nurse was observed and during the very first shift of observation, “this nurse gave a patient two aspirin tablets which were not ordered.” That wasn't all. Other errors she was involved in were:
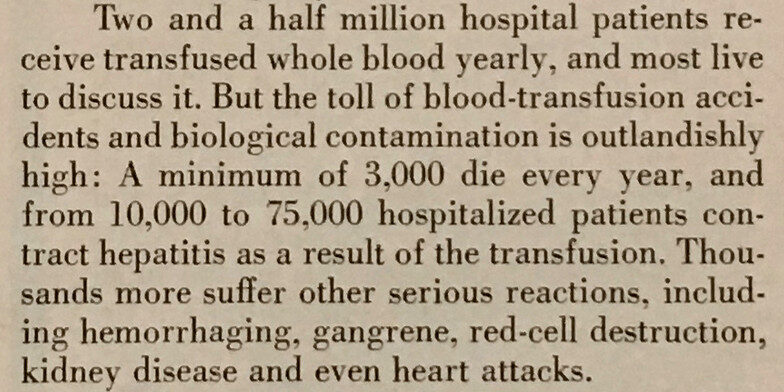
Blood Transfusion Errors
Blood transfusion errors were a much bigger problem in 1966, with at least 3,000 patients dying each year due to errors.
Rates today seem to be much lower in the U.S. and other Western countries, per this study.
I did not know this:
“Since 1976, the United States has required the reporting of all transfusion-associated deaths to the US Food and Drug Administration (FDA).”
This is still not the case for other medical errors, which get underreported or covered up far too often.
The 1966 article says:
… preventable “human failure” in the hospital accounts for at least 50 percent of blood-transfusion accidents.
Human error is to be expected. People are imperfect. If we're not blaming people for being human, we also don't just shrug our shoulders and act as if there's nothing we can do about human error. We CAN work to develop better, more robust systems that mitigate or prevent human error, as I blogged about here:
The 1966 article points out that many of the blood transfusions of the day (50%?) were unnecessary, which then unnecessarily exposed people to risk from transfusion error.
Lean today shouldn't be about doing the wrong things more effectively.
Other Accidents
One VA hospital study in the 1966 article “counted 3,747 nonmedical accidents among 108,005 patients” (3.5% rate) that included falling from beds (many “falling out of ill-designed hospital beds”), being “burned by chemicals and hot liquids, cut by thermometers, injured by equipment.”
Sponges and other items being left inside of surgical patients are still in the news today (including in England), as they were in the 1966 article.
These so-called “never events” are common enough that the problem perhaps inspired this TV commercial (that's not very funny when you realize this is a real and serious problem).
Maybe this serves as a much-needed comedy break:
But this really happens (in Jordan, 2015).
The Joint Commission is Mentioned
The author describes American hospitals as “a surprisingly free agent, answering virtually only to itself for its record of death, misadventure, and medical culpability.”
The piece continues:
“The external ‘control' is approval by the Joint Commission on Accreditation of Hospitals, whose criteria are both voluntary and generally unchallenging. Of 7,127 hospitals, 4,204 are accredited. Some 1,000 hospitals are too small to qualify, while many others blithely ignore the organization. A hospital's lack of accreditation should prompt suspicion, but approval is no guarantee of patient safety.“
I think that last sentence is still true today.
This article was written just one year after The Joint Commission received “deemed” status from Congress. The organization itself dates back to 1951.
A former Joint Commission chairman is quoted in the article as saying the “minimal” standards should not lead the public to “believe that accredited hospitals are ‘superior.‘”
But, today, the Joint Commission gives their “Gold Seal” to accredited hospitals, which seems to imply those hospitals are “superior.” Of course, how can most every hospital be “superior” when most of them manage to get accredited? Today, TJC says their accreditation implies “the highest standards for healthcare quality.” Hmmm. That topic could easily be its own blog post.
As a doctor points out in the 1966 article:
“… many hospitals go to sleep between [accreditation] surveys.”
Is that still a problem today?
By the way, the Joint Commission's mission statement was revised in 1999 “to explicitly reference patient safety” (see this slide deck they published). That's the year the report “To Err is Human” was published. Interesting.
Final Thoughts From the Article
The article concludes by saying:
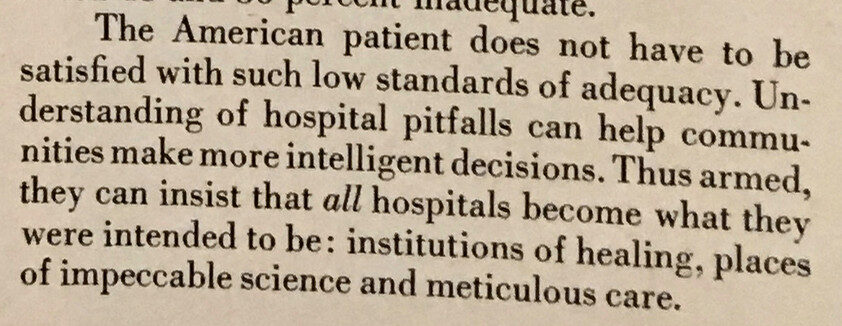
That's still true today, right? Patients shouldn't be satisfied with 2017's level of quality. We need to inform patients about risks, so they can better protect themselves (as the Batz Guide publications help with). We should make healthcare price and quality data more transparent and more easily available so patients can make better choices.
We are still working toward the goal of ALL hospitals becoming the best hospitals they can be.
What are your reactions to this look back to 1966? What are your thoughts about the progress that has been made (and, in some cases, hasn't been made) since then?
p.s. The author of the article, Martin L. Gross, wrote a book called The Doctors that was published in 1967. Time Magazine called it “incendiary!” as was proudly displayed on the cover of the book. This “Look” article was probably excerpted or condensed from that book. Gross later wrote a number of anti-government books with muckraking titles and also wrote The Medical Racket, released in 1998. So, I'm sure he styled himself to be a Ralph Nader type, but that doesn't make his analysis invalid. The ongoing patient safety problems get me fired up too.
What do you think? Please scroll down (or click) to post a comment. Or please share the post with your thoughts on LinkedIn – and follow me or connect with me there.
Did you like this post? Make sure you don't miss a post or podcast — Subscribe to get notified about posts via email daily or weekly.
Check out my latest book, The Mistakes That Make Us: Cultivating a Culture of Learning and Innovation:



 Bourbons")



{kind=link}
Comment from LinkedIn:
Hi Mark
Thanks for sharing this wonderful article…It shows where we were and where we are now. Infact many hospitals have not yet started the journey due to lack of intent or resources.
A headline from the UK about the lack of progress in one area:
Maternity ward blunders are as common as they were 20 years ago: Babies are just as likely to suffer brain damage through staff errors as they were in the late 90s
There are too many references to blaming staff instead of looking at systems and prevention.
Read more: http://www.dailymail.co.uk/health/article-4900742/Maternity-ward-errors-common-20-years-ago.html#ixzz4tvciMS48
Follow us: @MailOnline on Twitter | DailyMail on Facebook