


TL;DR: Lean isn't about turning hospitals into factories. It's about applying proven Toyota Production System principles–flow, quality, and respect for people–to healthcare settings like blood banks so professionals can improve safety, reduce delays, and redesign work together.
Today, I'm giving a talk at the International Society for Blood Transfusion (ISBT) conference in Toronto. I was invited by the company Quotient to participate in a panel discussion with laboratory professionals from the U.S. and the U.K.
The others are presenting examples of how they have improved flow, productivity, and quality in blood collection and hospital blood bank settings. Lean is often portrayed as just about efficiency or flow, but Toyota's definition of the Toyota Production System emphasizes that flow and quality go hand in hand.
I was specifically asked to give a short talk titled,
“What Do Cars Have to Do With Healthcare? How to Adopt and Adapt Lessons From Manufacturing.”
It's an intentionally provocative title on their part, and it's a topic I'm happy to discuss. Even though “patients aren't cars” and a “hospital isn't a factory,” Lean concepts apply because Lean and the Toyota Production System not just about building cars, as I've written about before.
We can adopt Lean concepts and adapt them to our environment as needed.
The other speakers and I are touching on key Lean points, including:
- There's a time and a place for automation… It's not a silver bullet, don't automate a bad flow
- Better flow can be achieved through smaller batches
- When key skills are in short supply, we need to be more efficient. We can work to reduce turnover by creating a better workplace environment.
- We can and should put safety and quality first.
- Safety and quality come through mistake-proofing, not double-checking… just as increased productivity comes through workflow redesign, not by telling people to work faster.
In my talk, I reference the brilliant 1989 NEJM article by Dr. Don Berwick, which I've written about before. You can find a PDF of the article online here, at least at the moment.
I shared a few highlights on Twitter in this thread:
Berwick draws a clear comparison between two types of factories that have two different management mindsets. One factory focuses on pressuring and frightening people through measurement, while the other factory has collaborative leaders who believe in their people and work to help them succeed.
One factory blames “bad apples” for quality problems, while the other factory focuses on systems and realizes that people want to do good work.
In his article, Berwick paints a clear picture of these two cultures… and how that second culture is what's needed in healthcare (when, today, almost 30 years later, too many healthcare organizations are like that first factory Berwick describes).
Hospitals are not factories. Blood banks are not emergency departments. Yet, Lean concepts apply in all of these settings. Lean is about helping the blood bank be the best blood bank it can be.
We could probably list more bullet points for what “Lean Blood Banking” would entail, but here are a few ideas. The one core theme in my section of the talk is how the “Respect for People” principle leads us to engage everybody in the continuous improvement and redesign of workflows.

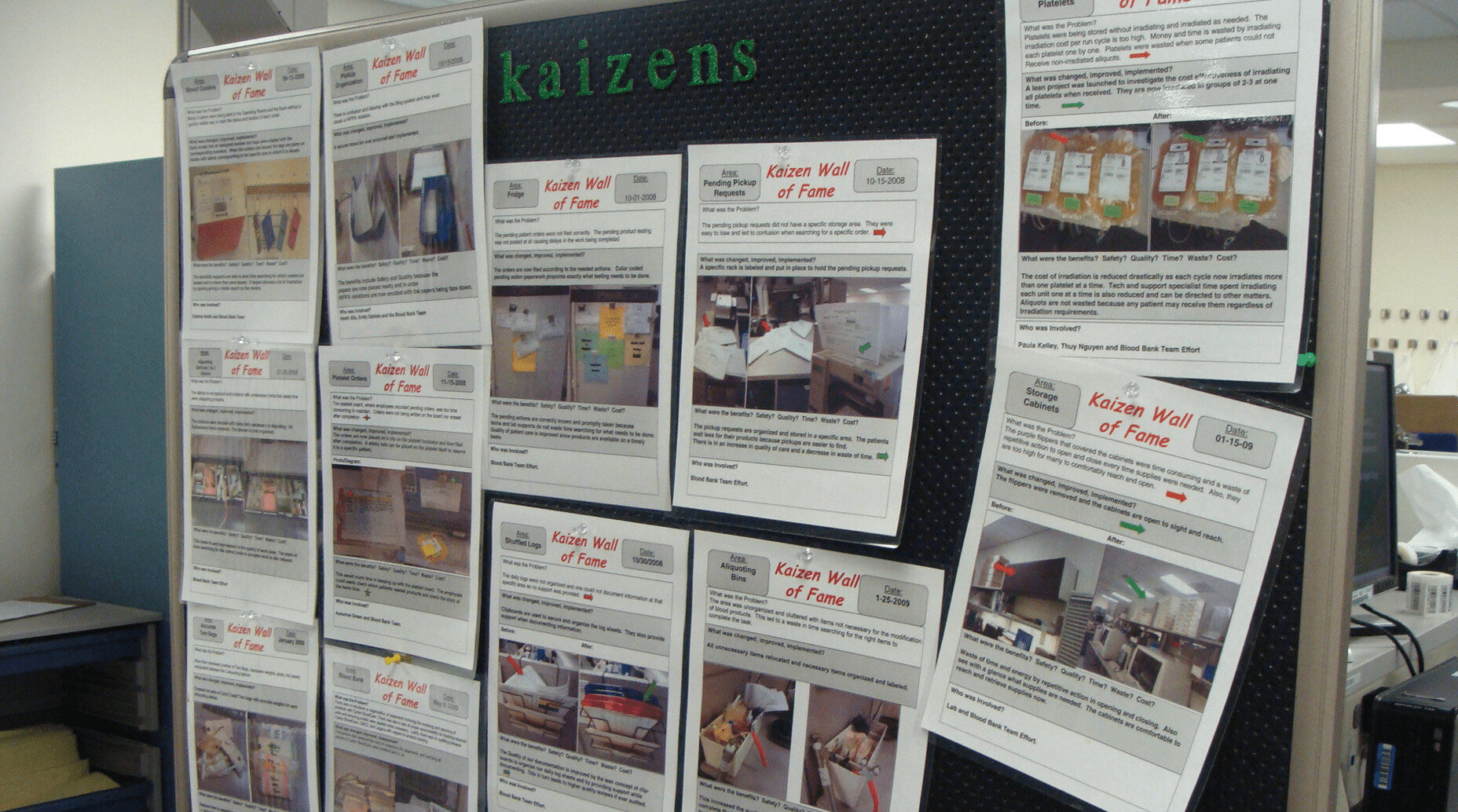
In my talk, I share examples from hospital blood banks that I have coached on “Kaizen” or continuous improvement. Their leaders engaged people to draw out problems and ideas for improvement.
“Small Kaizen” improvements don't require huge projects. It could be as simple as consolidating and organizing different paper forms that are used. One blood bank went from 145 different forms to just 37 (which still sounds like a lot, right?). That's an intermediate step, perhaps, before digitizing that process.
One blood bank decided it was better to irradiate all blood rather than do so “on demand” because the incremental cost was only slightly higher, and patients benefited from receiving blood more quickly (by pulling irradiated blood from stock instead of waiting for irradiation as needed).
One point I'll make in the talk is that the blood bank professionals are the experts. They are the only ones working in conjunction with other healthcare professionals in different departments to sort out the pros and cons of a change like that. My role is to be a coach and sometimes facilitator, not the one who is telling people how to improve.
So, as a blood bank engages people and solves small problems that matter, the number of improvements really starts to pile up. People see they are making a difference and they might feel more comfortable working on “Large Kaizen” projects, such as a more complete and systemic redesign of the lab or blood bank layout.
Anyway, I hope my talk is helpful today. I do encourage you to read the Berwick article and I'd be curious to hear what you think.
")



")

{kind=link}
Two tweets I sent with thoughts from other speakers:
Mark, I haven’t read your posts in a while and, reading this, I realize I need to get back into the habit of reading them regularly. What do cars have to do with healthcare? About as much as they have to do with law…which means you can adapt Lean to all those things. I wrote something similar back in 2014 (http://gimbalcanada.com/law-firms-car-rental-agencies-hotel-chains/).
I’m sorry I’m going to miss your talk – it applies directly to what we do. In fact, I could take some of your sentences and stick them directly into our work, and no one would be the wiser: solving the small problems that matter; using Lean to make the law firm the best law firm it can be; consolidating a huge list of forms (or contracts) into a few key standard ones…
But by far the one we use the most right now is almost word for word the same: automation isn’t the silver bullet people make it out to be. Fix the underlying process/flow problems before even thinking about automation. There is huge appetite in law for AI/automation/anything that looks like an easier solution than actually solving the process problems.
Thanks, Mark, for renewing my faith that Lean will work in any environment.