


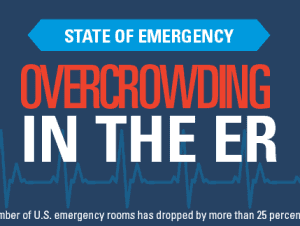
 Below is an infographic shared by the MHA program at the George Washington University Milken Institute School of Public Health.
Below is an infographic shared by the MHA program at the George Washington University Milken Institute School of Public Health.
There's some interesting data there… my comments:
The data on ED wait times shows only two data points (2003 and 2009). I'd like to see more data to draw a more valid conclusion about trends. It's unclear what the “wait” start and stop times are (since the average length of stay in the E.D. is usually a few hours). Billboards that advertise “average wait times” for the E.D. are also unclear… wait time until triage? Wait time until seeing a doctor?
Of course the average wait time in an E.D. “with boarding” is going to be longer, since boarding (keeping an admitted patient in the E.D.) is a sign of poor end-to-end patient flow (caused by not having inpatient beds available, through no fault of the E.D.)
Where it says “solutions,” I'd argue that “reduce E.D. boarding” is a goal. The exact solution or solutions would take a lot of root cause analysis, problem solving, and implementation of ideas.

Brought to you by MHA@GW: MHA degree
What issues do you see in your hospital related to E.D. overcrowding. What are you doing about it?
Please scroll down (or click) to post a comment. Connect with me on LinkedIn.
Let’s work together to build a culture of continuous improvement and psychological safety. If you're a leader looking to create lasting change—not just projects—I help organizations:
- Engage people at all levels in sustainable improvement
- Shift from fear of mistakes to learning from them
- Apply Lean thinking in practical, people-centered ways
Interested in coaching or a keynote talk? Let’s start a conversation.







{kind=link}
All the listed facts and figures are well chronicalled in the literature. I’ll comment on 3.
1) Lack of access to other viable options to be seen- primarily ‘after hours’and weekend/holiday availability; and their doctor cannot see them in the time frame they feel is needed
2) 50% ED’s operate at or over capacity- not every minute but often on any/every given day
3) the increasing number of behavioral health patients held in ED’s for hours/days/even weeks.
#1- we have a system that asks the least experienced person- the patient (or family)- to triage their issues in determining when and where to seek care. Is there any wonder this doesn’t match up to the capacity/availability in the system? This is not the patient’s fault, but needs to recognized to best deploy the resources the system has.
#2 &3- In each instance, operational decisions by the hospital challenge the ability of the ED to manage flow. In each instance, the hospital often makes these decisions based on its financial accounting system, which is often not capable to identify true costs of care, which skews the other impacts on quality, safety, flow and morale, that are given less weight in the decision.
For instance, there are examples of what happens when the mental health patients are not kept in the ED and the resultant markedly improved effect on ED flow and performance; yet, hospitals make the decision to keep them in the ED. There is no mandate that this is where they must be kept. It is a conscious institutional decision.
Same with operating at capacity, ie, not having adequate capacity to meet the demand. There are clear patterns of patient arrivals over a 24 hour period, day or week. But these do not reflect the reality of the experience, which is determined by the unpredictable hour by hour variability of arriving patients and the insufficient capacity to move them through expeditiously and appropriately during influxes, leading to backup. The median/average of metrics used do not give an accurate picture of this effect– which is why sometime you can walk through the ED and not much is going on (ie, we are wasting money on staff we don’t need) and other times, it is way overstretched (why don’t you just work harder and faster).
‘Where it says “solutions,” I’d argue that “reduce E.D. boarding” is a goal.’ Mark, yes, we confuse goals, metrics and solutions.
‘The exact solution or solutions would take a lot of root cause analysis, problem solving, and implementation of ideas.’
This would require a level of collaboration, trust and shared intentions that are hard to come by still in many, if not most, healthcare institutions.
Continuous improvement is built upon the respect for people principle. And when not, that may be the real root cause why the pace of change is increasing, but the pace of improvement not so much.
I look forward to more comments on this blog post- Mark