


Update Nov 5 7:30 pm: Added an Addendum / Epilogue to the story at the end of the post
Having received a Johnson & Johnson vaccine in March (at Dodger Stadium), I was happy to have the opportunity to get a booster. Based on data from a study that suggested that a Moderna dose on top of the J&J dose provided the strongest antibody levels (and after talking with a physician), I decided to get the Moderna shot on Tuesday.
Scheduling through the nearby CVS was easy enough. But the customer experience really went downhill once I arrived at the store.
I started writing this blog post on Tuesday night when I thought the story was just about “a disorganized waiting process.” But, by Wednesday afternoon, I realized that I was victim of a preventable “vaccine administration error” — thankfully, one that didn't cause any harm to me.
I'll tell the story, but a few hours after the injection, I got an automated request for feedback from CVS. I've blacked out the store location for my own privacy and to keep the focus off of “what's wrong at that store?” when these are likely systemic problems across CVS locations — or at the least, the culture is most likely driven by CVS corporate leadership.
In most customer satisfaction “likely to recommend” surveys, if you don't give a 9 or 10, it's all considered a fail — so I think I clicked 3, as it doesn't really matter.
But, CVS did ask for free form feedback in a paragraph text field. They also invite you to record a video giving feedback (that's new to me), but I figured I would write a blog post and then just send them the link in that feedback field.
If they care. And I'm not sure that they will.
Before Arrival to CVS
I got some helpful automated reminder text messages from CVS, with links to useful information. About 90 minutes prior to my appointment, I got another text:
On my way to CVS, by foot, I got about 10 steps outside of my building and realized, “Oh, I forgot my CDC vaccination card.”
SUGGESTION #1: Put that into the reminder — “Bring ID, insurance card(s), face covering, vaccination record card.”
It turns out my insurance cards (one for medical and one for pharmacy) were NOT required. So maybe that could be removed from the reminder text.
Hear Mark talk about this experience in a bonus episode of the “My Favorite Mistake” podcast:
Arrival to CVS
I arrived ten minutes early (at 4:20) as I had been instructed to do. Being familiar with this store, I figured I would walk back toward the pharmacy area, as that's likely where the vaccines were being given.
I saw a huge sign that, at first, seemed helpful.
Here for my COVID-10 vaccination? YES.
Proceed to the vaccination area? OK, WHERE?
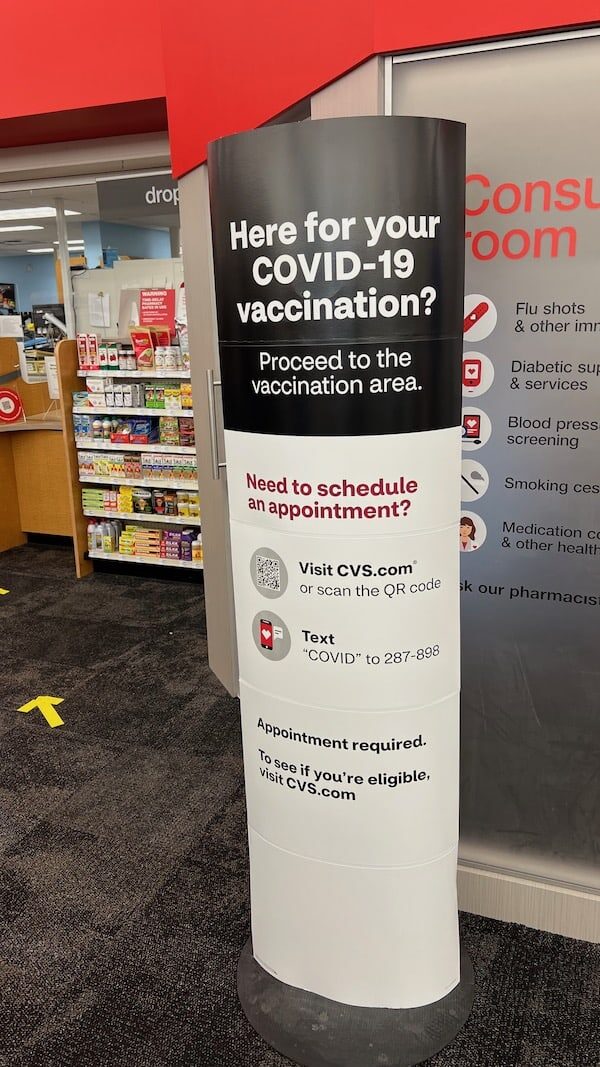
SUGGESTION #2: Put an arrow on the sign telling us which way to go.
The Minute Clinic area to the right? The pharmacy area to the left? This was really unclear. So, I looked around and saw people in an area to the left of the pharmacy pick up area, so that seemed like it.
I walked over and saw a yellow sign taped up to the wall saying it was the “VACCINATION AREA.”
There were a number of chairs in the area, spaced out a few feet apart. Maybe six feet. I didn't measure them.
I sat down.
There were seven or eight people apparently waiting for their vaccine — flu shot, Covid, or maybe both.
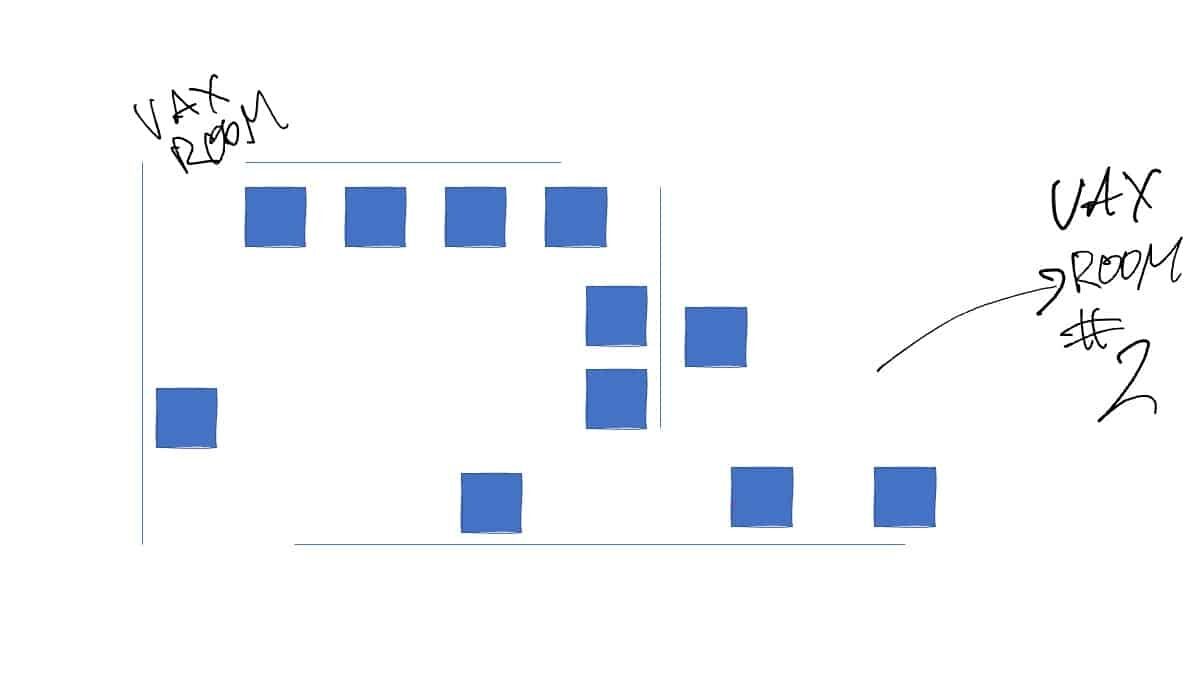
The area looked roughly like my sketch below. I wasn't about to take a photo of an area with patients in it.
Getting Yelled at For Not Understanding Their Process?
A woman came out (a manager?) and started chastising patients / customers for not lining up properly for the vaccination.
She very gruffly pointed out that we were supposed to be seated in sequence. That the chairs formed a queue.
“How were we supposed to know that?,” said one patient.
SUGGESTION #3: Have a greeter to explain the process to people who arrive.

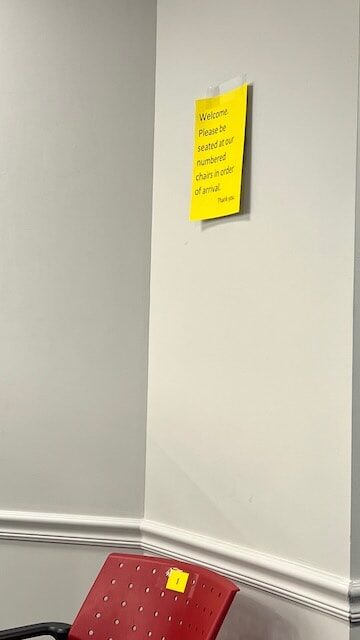
The chairs (most of them) had small numbers on the chairs, as pictured here.
“Why aren't you just taking people in the order of appointment times?,” asked another patient.
It was really not obvious that the numbers meant a queue sequence.
There WAS a tiny sign, but I hadn't seen it, nor had many others. It said, “Welcome, Please be seated at our numbered chairs in order of arrival.”
SUGGESTION #4: Post the sign at the ENTRANCE to the area.
SUGGESTION #5: Make the language more clear.
The woman explained that we needed to move from chair to chair as the line moved along. It was sort of a game of musical chairs. Thankfully, we're less concerned about touching surfaces these days, as we've learned more about Covid.
The layout of the chairs didn't make it obvious there was a queue formed. The chairs weren't in a straight line, at all.
“Well, it's better than standing!,” the woman barked at us.
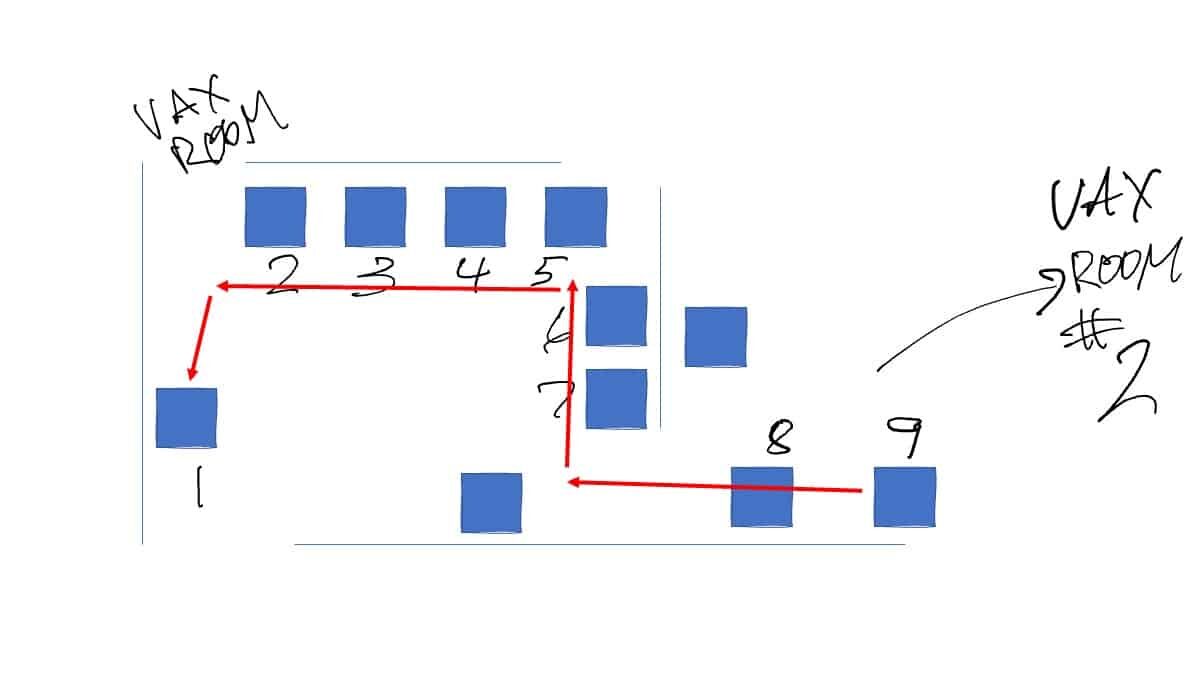
Again, two of the chairs weren't numbers for some reason. This was not the least bit obvious.
GENERAL LESSON: Don't blame your customers for not understanding your unclear process.
Getting Called Back to a Vax Room
Once I had moved along to Chair #1, a pharmacist came over and told me to follow him to the consultation room (what I labeled Vax Room #2).
On the way over, he asked, “Were you checked in?”
I said, “Yes, I tapped the link on the app as I was instructed to do.”
“Oh, that's not really the check in.”
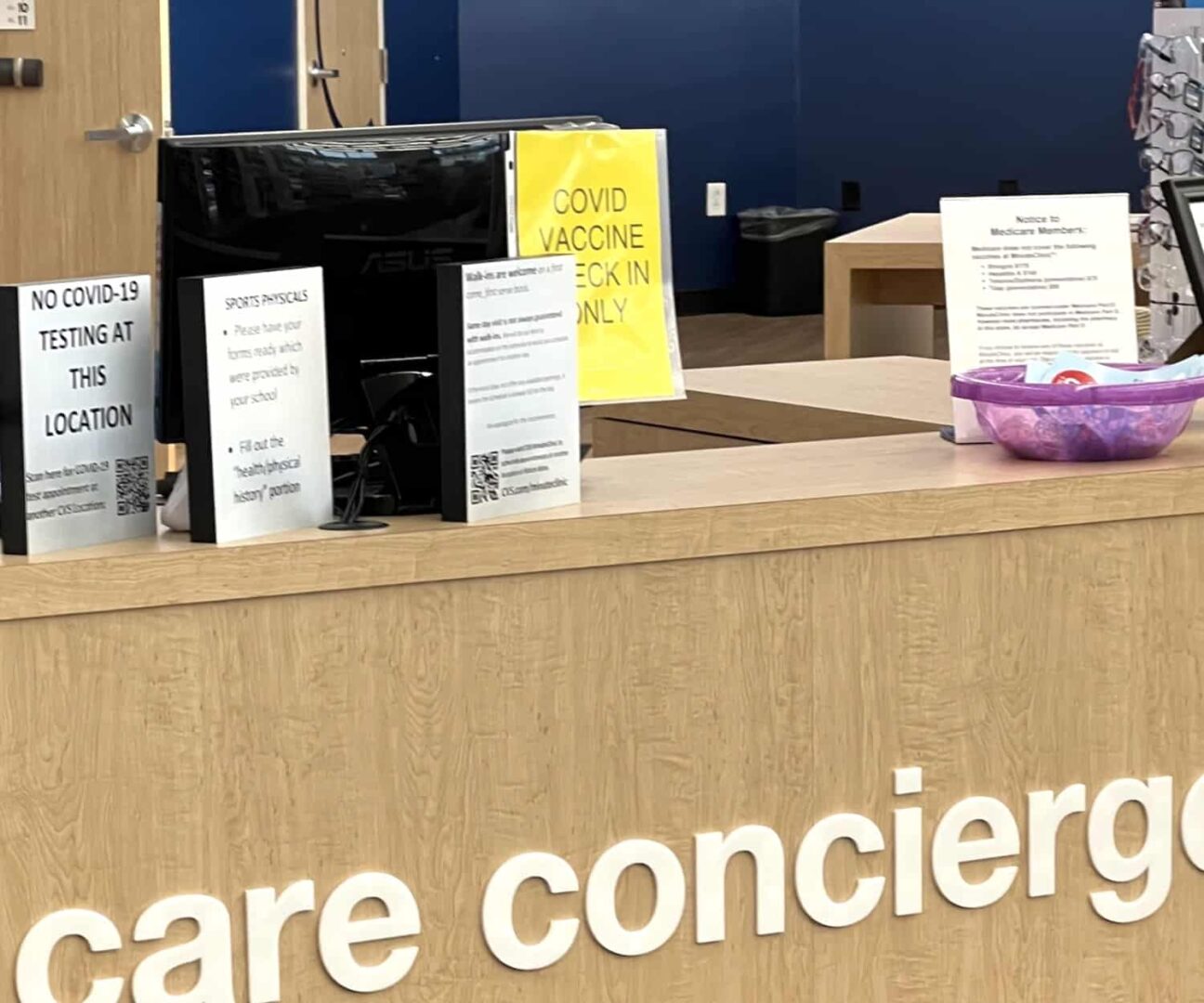
Apparently, the HealthHub clinic area had a check in step at their desk. I didn't notice the yellow sign because I had read the BIG sign that said
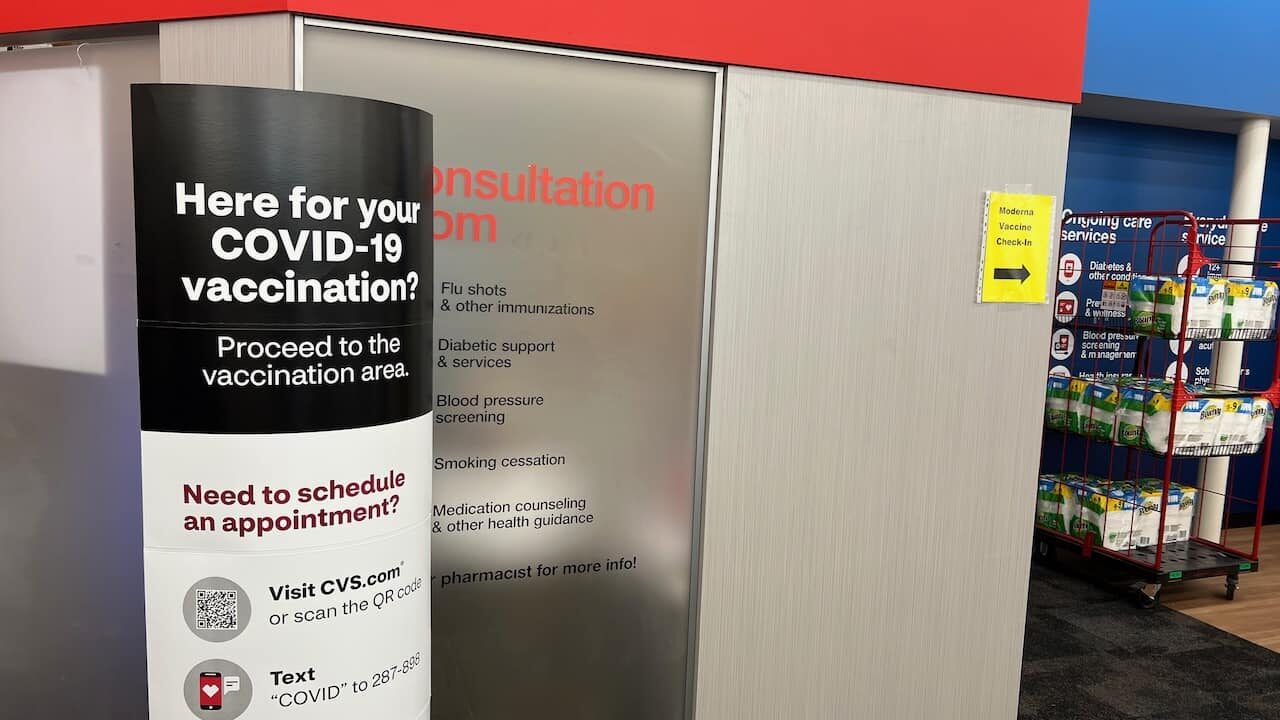
SUGGESTION #6: Have the big free standing sign say “Proceed to the check in desk” OR put the yellow sign on the big floor standing sign instead of on the wall.
I had totally missed the check in station sign on the desk because I didn't even look in that direction, to the right.
The pharmacist then took a minute or so inside the consult room to get me “checked in” via an app he was using on a mobile device.
The Vaccination Was Given — Turns Out There Was an Error
As I shared yesterday, in my post about vaccination errors, I was the victim of a vaccine dosing error. I didn't realize this until the day after vaccination.
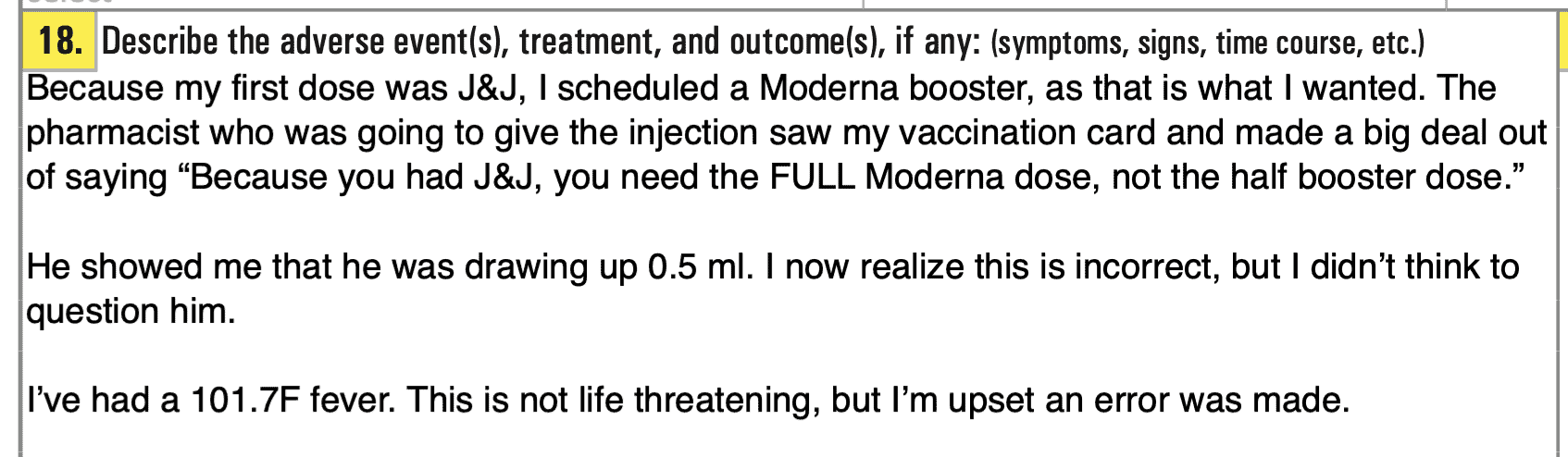
The pharmacist looked at my CDC vaccination card, which said I had gotten the single dose J&J vaccine in March.
He said, “Oh, because you had the J&J, I have to give you the full dose, not the booster dose.”
I did not even think to question this since he's supposed to the expert. Or, he's supposed to be trained and educated sufficiently by his employer, CVS. These are all systemic problems — I'm not blaming this individual.
He was again talking me through his process, that he was going to draw up 0.5 mL of vaccine (a full dose) instead of the 0.25 mL “booster” dose.
I saw him draw up 0.5 mL into the syringe and he was making a point of letting me see that. Which I thought was good.
The injection wasn't painful. The pharmacist was pleasant and seemed happy to help. He didn't seem rushed or stressed, which was good. I'll come back to the error in a minute.
As with my initial vaccination at Dodger Stadium, I was not given any information about side effects to expect, who to call if I have a problem, etc. I think my wife got a helpful info sheet when she was vaccinated the first time.
SUGGESTION #7: Have post-vaccination instructions for the patient. Even if it has a QR code or a website link (because we have to account for different languages).
Trying to Give Some Feedback — Nope
The woman who yelled at us for not following their unclear process then saw me. I had to do the 15-minute observation wait, but I had a medication to pick up and there was a long line for that. So, I decided I could stand in line instead of going and sitting down in the observation area.
Nobody told me not to do that.
The woman seemed confused about why I was standing there, and she asked, “Did you get vaccinated?”
I told her I did and, at that point, I had figured out that I had missed the signs. I tried explaining calmly that the signs, and the whole process, was confusing. Maybe you should put the sign about going to check in on the big floor-standing sign.
I could tell she was NOT interested in really hearing my feedback or doing anything with it. Again, I'd consider that to be a systemic CVS problem. I'm not blaming her individually. Her behavior is likely the product of a system, one that might have her overworked (she seemed stressed and agitated).
The Next Day
When I got the J&J vaccine, I had some very minor side effects the next day. I had a low-grade (just under 100 F) fever for four or five hours. I napped it off. My fever broke. I felt normal that evening.
Remember, these short-term side effects are NOT harmful — they're actually a good sign that the vaccine is working (your body is responding).
Wednesday, the day after getting the Moderna shot, it really started hitting me at about 9 AM. I had blocked off most of the day to not have meetings — a luxury that I have with a work at home job with flexible hours. My last meeting was ending at 9… and I took my temperature and it was again about 99.5.
I went back to bed, expecting to rest and nap it off. By about 3 pm, I thought the fever was breaking because I felt warmer. Turns out, my fever was going up to about 101.9.
I started wondering… my gut said, “Maybe the pharmacist wasn't correct about the dose.” I've been around healthcare long enough (16 years) to know that medication errors are a big problem — in hospitals, clinics, and pharmacy settings. Remember, I had already blogged about various vaccine process errors that had occurred around the world.
I rested some more and I was fretting a bit. I knew, from the cases where people were mistakenly injected with a full un-diluted vial of the Pfizer vaccine, that getting a 5x or 6x “overdose” wasn't harmful. So, If had had incorrectly gotten 2x the booster dose, I knew I wasn't in danger.
But, given that I work with healthcare organisations on systems improvement (to the benefit of safety, quality, and more)… and the fact that I host a podcast called “My Favorite Mistake” meant it was pretty ironic that I was potentially the victim of a medication error.
As I said at one point yesterday, “If I'm destined to be victim of a medication error in my life, I'll take this one.” Sadly, medication errors are so common that I'll likely face another one in my lifetime.
I Started Researching
I found a reputable source that told me that my pharmacist was incorrect and misinformed — the CDC website.
There's a four-page PDF document that has instructions about giving the boosters.
It seemed pretty clear:
All persons who received a single dose Janssen COVID-19 Vaccine should get a booster dose of a COVID-19 vaccine at least 2 months (8 weeks) after receiving the primary dose.
That included me. So what is a “booster dose”? You have to go to the next page…
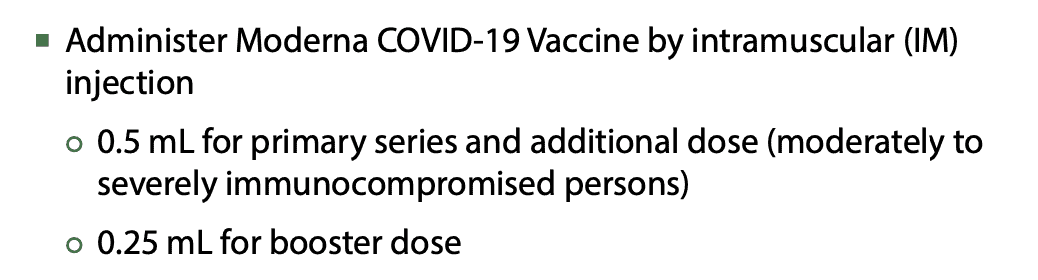
I'm not immunocompromised. The pharmacist hadn't brought that up as a reason for giving me 0.5 mL. Remember, he said it was because I had gotten the J&J. But that's wrong.
The booster dose for ALL non-immunocompromised “fully immunized” people (which included me with my single J&J shot) was to be 0.25 mL.
This same mistake has happned with patients:
Calling the CDC
There is a CDC hotline that you can call with questions. So I called. I got through to a human pretty quickly and easily. I explained what had happened.
She said, bluntly:
“That is no good. That is the wrong volume.”
The woman on the phone said that I had a “vaccine administration error” to report. I could report this via another phone call or a PDF form. I chose the PDF form and filled it out. Uploading through the website (option 1) didn't work for some reason, so I emailed it to them (option 2).
About 20 hours later, I've gotten no confirmation that my VAERS report was received.
EDIT: See the post comments, below, for an article that I found from October 21 that talked about the risk of confusion due to the Pfizer booster being a full dose and the Moderna booster being just a half dose.
Calling the Pharmacy
I tried calling the CVS store because I felt obligated to let them know about the error. I was a bit afraid that my pharmacist would get in trouble — that wasn't my intent and, again, I see what happened as a systemic problem. There are likely to be at least some misinformed pharmacists at various CVS sites around the country.
But, it was impossible to reach a human. Going through the Voice Response System a few different ways, I would either get disconnected when it started ringing through to a person after a few minutes of hold music. Or, it would strangely kick me over into a voice mail system, it would read an error message, and ask me to enter my mailbox number.
Oops.
Calling CVS Corporate
I had the energy to call CVS corporate customer service. Again, I figured that, had I been able to reach the store, they wouldn't have a culture of reporting errors and problems upward through the leadership chain.
I wanted CVS corporate to know his error had occurred and that they should make sure it wasn't happening in other stores.
I had to wait on hold 45 minutes, but I finally reached a real person. She was very helpful. She listened to my story, understood what the problem was… but then after taking notes, the only “resolution” was that I would be contacted by somebody within “24 business hours” — which could mean NEXT MONDAY.
We'll see if that call to corporate meant anything.
SUGGESTION #8: CVS should act with urgency and communicate, by the next morning, to ALL stores that this error occurred. Awareness doesn't prevent problems, but it's a good first step.
Update November 8, 4 pm PT: I did not get a call back within 24 business hours.
More Information From Doctors
I talked to a few friends who are doctors, including Greg Jacobson at KaiNexus and a college friend.
They pointed out a few facts that were reassuring… and, again, I wasn't really worried about getting the extra dose — I was just annoyed.
- One doctor told me that this error might, ironically, work out to my benefit (better protection)
- Another doctor told me that the Moderna booster trials were done with the “full” dose of 0.5 mL
The safety and efficacy of the booster was proven based on the full dose — the dose I received. It was later decided that the half dose provided enough protection to be worthwhile.
So, good for me. I'm “super vaccinated”? My words, not the doctors. I know the booster, just as with the original vaccination, doesn't mean I can be reckless. Just because I have an airbag doesn't mean I'll drive recklessly without a seatbelt on.
Going Back to CVS
Since I couldn't reach the store by phone, I walked over there this morning at about 10 am, when I figured the pharmacy manager might be there.
I made a point of wearing my “ZERO” hat from the Patient Safety Movement Foundation (you can see a photo of it in this blog post).
I asked to talk to the pharmacy manager. He came over and I explained what happened.
He recognized the error right away.
“Did you mark off in the app that you're immunocompromised?”
No, I did not. Or, I'm quite certain I did not and that wasn't mentioned to me by the pharmacist as a reason for giving the full dose.
The pharmacy manager didn't argue with me. He believed me. He apologized.
He said:
“That pharmacist comes in later today, so I'll talk to him.”
SUGGESTION #9: Don't write up or punish the individual pharmacist or pharmacy location. Look at the systems and processes related to training and education.
Does CVS Have a Climate of Psychological Safety?
I wrote a blog post recently for the Value Capture blog:
Psychological Safety and its Essential Link to Continuous Improvement
To have the highest levels of performance, we need psychological safety in the workplace. If you're unfamiliar with the concept and the research that proves this, listen to my podcast with Professor Amy Edmonson from Harvard Business School on the subject.
I've tried to emphasize that I do not blame the pharmacist. The pharmacists all work in a system. Senior leaders (at the store, district, and corporate level) are responsible for the systems and the culture.
Did the pharmacist have the psychological safety to ask:
“Hey, I'm not certain which dose we give to the J&J vaccinated, what should I do? How do we confirm this? How do we make sure everybody knows?”
Or:
“Hey, I think I just made a mistake and gave the wrong dose. What should we do?”
I'm just guessing… but I am guessing the pharmacists do not have psychological safety. The woman who was being rude to the customers… does she also talk to employees that way?
What Would Toyota Do?
I ask this question because of the roots of Lean being at Toyota, of course. I also ask it because I had the chance to visit two amazing mass vaccination sites, in San Diego and the Dallas suburb of Frisco, where former (or current) Toyota people helped design, manage, and improve the process.
Those sites ran smoothly. Now, both of those had the advantage of being in dedicated spaces that no other responsibilities than vaccination.
That said, we always have a responsibility to intentionally design an effective process. Maybe CVS doesn't have that skillset. Did they allow the process to “just happen” (meaning it wasn't really designed) or did they design it badly? Either way, will CVS improve it?
The original title of this post was “This Vaccination Process Was Clearly NOT Designed by Toyota People.” I wish it had been.
I'm convinced that if Toyota ran a pharmacy location or chain, they wouldn't have stressed out, overworked (and sometimes understaffed) conditions. They'd find a way to be profitable by having the right staffing levels for the work and to provide the highest quality of service and care.
You might want to listen to this week's podcast about Lean process design, with my guests Matt Zayko and Eric Ethington.
What Would Alcoa Do?
Why does this question matter? Well, Alcoa and the late Paul H. O'Neill, Sr. had an amazing track record on safety (and other measures of corporate performance, such as the stock price) during his tenure as CEO (and beyond).
One habit was to make sure that safety alerts were communicated quickly throughout the company, throughout the world.
I asked Ken Segel, CEO of Value Capture about this (he knew O'Neill quite well), asking this question:
I'd be curious to hear your thoughts about “what if Alcoa ran this pharmacy”?? How quickly would this one error (once I reported it to CVS corporate) lead to swift communication out to ALL CVS locations about the opportunity for error?
Ken said:
I think the answer to your question is “immediately.” I heard Paul ask people on the floor in healthcare more than once, “How long does it take for that knowledge to go to everyone else who does your job anywhere in the hospital, health system, country?” And “why not instantly?”
Will the CVS pharmacy manager share what happened with pharmacists other than “the one who made the error”? Will they report the error up the chain? Is it safe for them to do so? Again, probably not.
But, I hope CVS would have the culture and the systems in place to spread knowledge of this error INSTANTLY across every CVS location. Why not share this with EVERYBODY in the pharmacy field?
To learn more about the Alcoa / O'Neill approach (including the applications to healthcare), check out the free eBook titled “A Playbook for Habitual Excellence: A Leader's Roadmap from the Life and Work of Paul H. O'Neill Sr.”
Reflections and Conclusions
So, that's my medication error story. I feel fine today. I'm glad the error wasn't harmful. But the “wrong dose” error goes into the category of so-called “Never Events.” I say “so-called” because they happen far too often, even after this hopeful term was first used 20 years ago.
It's a Shouldn't Event. It's a Wouldn't Happen Event if we had better systems — a better culture, a better management system, etc.
I hope CVS learns from this error and applies the learnings in a way that can prevent a future similar error (with another class of medication) that might cause real harm to a patient.
I know I put Toyota up on a pedestal, but I'm very confident that this error wouldn't occur if it were a Toyota-run pharmacy…
One other thought I had… when I saw how chaotic the process was, from a signage and waiting perspective, along with the attitude of the woman who sorta yelled at us, I wonder if that should have given me pause about the clinical quality. Is “poor customer service” a more visible indicator of “poor clinical care”?
In hindsight, maybe I should have bailed and gone somewhere else. But, as I learned, it was better to get the “double” dose without delay than it would have been to wait another day or two for the correct dose.
Epilogue: Follow Up and Improvement
To my pleasant surprise, I got a call late Friday afternoon from the pharmacy manager I had spoken to in person.
He told me that he had talked with the pharmacist and that the individual had already come to the realization that he had the wrong understanding about the booster dose. It's unclear to me (and maybe doubtful) if he would have felt safe bringing that up to the manager unprompted.
Thankfully, the manager didn't say anything about punishment — as I don't think it was merited.
The manager reiterated that this was a “serious error” and that it shouldn't have happened. He did talk to other pharmacists to make sure nobody else had that incorrect understanding. He also talked to his district manager to run it up the chain for broader communication.
I thanked him for that follow up and asked him if he had a minute to hear some other feedback. He said, “Sure.”
I told him about the musical chairs, and the poorly located / unclear signage.
Regarding the chairs, he said they had realized that was not working, so they removed the chairs and just have a traditional standing queue and that's working better — great!
He also took to heart my feedback about the signage related to check-in and more — he said they could make some improvements around that.
So, at least they are learning and improving. I just hope the lesson spreads to other CVS locations and beyond.
Please scroll down (or click) to post a comment. Connect with me on LinkedIn.
Let’s work together to build a culture of continuous improvement and psychological safety. If you're a leader looking to create lasting change—not just projects—I help organizations:
- Engage people at all levels in sustainable improvement
- Shift from fear of mistakes to learning from them
- Apply Lean thinking in practical, people-centered ways
Interested in coaching or a keynote talk? Let’s start a conversation.







{kind=link}
Here is an article from October 21:
Half doses, third doses, kids’ doses: Covid vaccine delivery goes next-level difficult
I realize that people are exhausted, but this isn’t rocket science or brain surgery… with good process, you could manage all of this complexity just fine.
I agree:
This seems like the right approach:
Mark: Based on your observations, it appears that not only did the pharmacy design-in plenty of waste (muda) with the door-to-door booster process, but they also set up a process that was very unreasonable (muri) from the viewpoint of the users (patients)–an example of this based on the need for “musical chairs” for indexing in the queue. So much potential touzen in the process that could keep the “improvement” team busy for awhile. Thanks for sharing the experience in a detailed manner.
A story that was shared with me by a friend:
Why are CVS employees yelling at customers for being confused by their confusing set up?
I was told, by the person on the phone at CVS corporate, that somebody would call me to follow up within 24 business hours. That did not happen.
They never called me.
More errors (at least those that made the news):
Sutter Health Admits To Giving Wrong COVID Vaccine Dosage To 14 Children at Antioch Clinic
Nearly 100 students receive wrong COVID vaccine dose in Montgomery Co. clinic
Both cases cite “human error” which is, of course, not really a root cause. There are failures of processes and systems… which is why we need effective training, solid processes, and error proofing. Don’t just shrug your shoulders at “human error.”
Virginia pharmacy gives 112 kids wrong doses of COVID vaccine