

Eight Types of Waste in Healthcare: Real Examples from Hospitals
TL;DR: Nurses typically spend only 30% of their time on direct patient care. This post walks through the eight types of waste in healthcare — with real hospital examples — and how Lean methods have helped some organizations reclaim that time.
What are the problems and annoyances that constantly appear, interfering with our work and the best patient care? In Lean, we call this waste. Dr. Don Berwick describes waste as a “needless hassle” and “what does not make sense in our health care system.”
Why Reducing Waste Matters
Hospital employees typically spend a high percentage of their time on wasteful activities. For example, medical/surgical nurses in hospitals around the world typically spend only about 30% of their time on direct patient care, including:
- Nursing procedures
- Hygiene and toileting
- Administering medication
- Giving medical guidance
And the studies that generated those results were done before the widespread adoption of electronic medical record (EMR) systems. EMR systems may solve some problems, but new technologies sometimes create new forms of waste and keep providers away from the bedside even more than before.
When employees, departments or hospitals are overworked, we need to reduce waste instead of just asking for more resources and people. Reducing waste, by improving processes, also allows us to take on more work without adding people, doing so in a way that does not stress our employees. Reducing waste also provides time for people to do their work the right way–providing high-quality and great service to patients instead of being pressured to cut corners due to a lack of time. Eliminating waste allows us to reduce costs, provide more service, improve quality, and improve employee satisfaction–it is good for all of our hospital stakeholders.
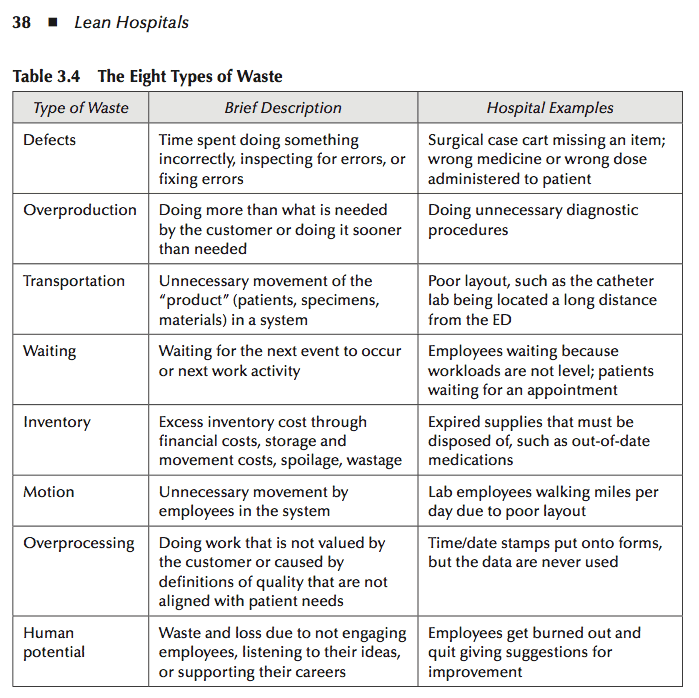
To help identify waste, having specific shared terminology can help. Ohno defined seven types of waste, while later publications often listed eight types. These definitions have been adopted as a useful framework for viewing waste in hospitals. Sometimes, the terms are used verbatim; sometimes, they are modified. Having complete agreement on the exact terms is not crucial, as Toyota did not intend this list to be all inclusive or to be something that could not be changed. Consistent terminology does, however, help us communicate within our organization and across the industry.
Hospital workdays are full of interruptions, miscommunications, wasted motion, and workarounds. When supplies are missing, we run to find them. When workspaces are badly designed, we walk faster and try harder. When orders don’t arrive from a physician’s office, we make multiple phone calls to track them down. It’s good, in a way, that people make this effort. But they shouldn’t have to. These workarounds don’t prevent the same problem from happening again tomorrow.
The DOWNTIME mnemonic. Many Lean practitioners remember the eight wastes through the acronym DOWNTIME: Defects, Overproduction, Waiting, Non-utilized talent, Transportation, Inventory, Motion, and Extra-processing. The order below follows Ohno’s original sequence rather than the mnemonic.
Learning to separate motion (the things we do) from value (the things we do that help the patient) is a critical step. Lean gives us a framework for seeing that difference clearly — and a shared language for talking about it.
Taiichi Ohno at Toyota originally defined seven types of waste. Later publications added an eighth: wasted human potential. These categories aren’t meant to be rigid or exhaustive — Toyota never intended them that way. They’re a starting point for seeing work differently.
The examples below are drawn from my book Lean Hospitals and from real organizations that have applied these ideas.
Defects
A surgical case cart arrives in the operating room missing an instrument. A patient receives the wrong dose of a medication. A form gets filled out incorrectly and has to be redone. In healthcare, defects mean any work not done right the first time — including the time spent inspecting for errors and fixing them. Some defects are minor inconveniences. Others injure or kill patients.
At one hospital, the anatomic pathology lab couldn’t always find tissue slides that needed re-reading. When a slide went missing, technicians had to locate the original tissue block, recut it, and start over — more time, more labor, more cost, and more delay for the patient.
Overproduction
Studies show that 20 to 50 percent of hospital lab tests are completely unnecessary. At the University of Utah Health Care, the hospital started requiring residents to justify each test and saved $200,000 a year. At one hospital pharmacy, 480 medications were returned to the pharmacy every day — more than one per admitted patient — because orders had changed or patients were discharged before the medications were administered. Pharmacy staff spent 11 hours a day processing those returns.
Overproduction means doing more than the patient needs or doing it sooner than necessary. In healthcare, that includes unnecessary diagnostic procedures, “just-in-case” blood draws that go unused more than 90% of the time, and the overproduction of reports nobody reads. One hospital’s chief clinical officer discovered more than 320 different reports being generated daily or annually, with no formal process for deciding whether any of them were still useful.
Transportation
One hospital used Lean methods to follow a 74-year-old woman from arrival to surgery. During the course of her visit, she walked the equivalent of five and a half football fields. Transportation waste is any unnecessary movement of patients, specimens, or materials through the system.
Park Nicollet Health Services in Minnesota designed its Frauenshuh Cancer Center so that patients stay in a single room for nurse and doctor visits, lab draws, treatment, and other support services. The care comes to the patient instead of the patient walking between departments.
Waiting
Patients wait for appointments, for test results, for a bed to open up, for discharge paperwork. But employees wait too — for information, for equipment, for the next patient to arrive. At one neurology department, all but the most urgent patients waited a long time for an appointment, even though the neurologists often concluded the referral had been unnecessary. Each inappropriate referral meant a patient who actually needed the consult had to wait longer.
Waiting is time when nothing value-added is happening. It is probably the most visible type of waste in any hospital.
Inventory
Expired supplies sitting on shelves. Out-of-date medications that have to be disposed of. Surgical kits that contain instruments the surgeon never uses — sterilized repeatedly and never opened.
In one hospital, a central supply cabinet system led nurses to hoard supplies in drawers, lockers, and pockets because the cabinet was inconvenient to access. The hospital started reconsidering which items truly needed tight control and which could be stocked closer to the point of care. The trade-off matters: if items are inexpensive and don’t take up much space, storing them in more locations often reduces total waste in the system.
Motion
Medical-surgical nurses in hospitals around the world typically spend only about 30% of their time on direct patient care. Much of the rest goes to walking — searching for supplies, hunting for equipment, traveling between workstations, and navigating workarounds in electronic medical record systems.
In one hospital, lift assists for patients were stored in a closet on a different floor because the unit didn’t have enough storage space. Because it was inconvenient and time-consuming to go get the proper equipment, nurses often lifted patients without the assist — increasing the risk of employee injuries and patient falls. The unit used 5S to free up space and relocated the lifts, reducing walking and ensuring the right equipment was actually used.
Seattle’s Virginia Mason Medical Center has used Lean methods to increase nursing time at the bedside from about 33% to 90%. The National Health Service in the United Kingdom has taught Lean methods to nurses and hospital staff through its Releasing Time to Care program. On average, time at the bedside increased from 35% to 55% across 19 NHS Scotland hospitals that implemented the program. Hospitals in the United States are using a similar approach called Transforming Care at the Bedside (TCAB), which sets a goal of increasing bedside time from 30% to 70%. One system that adopted TCAB reported the time nurses spent in patient rooms increased from 2.5 hours in a 12-hour shift to 6.5 hours, resulting in a 32% reduction in falls and a 17% reduction in medication errors. Nurse turnover rates in TCAB hospitals fell by nearly 20%, suggesting that an environment with less waste and more time for patient care is more rewarding for staff.
Overprocessing
In one hospital’s surgery department, an employee spent three hours a day folding towels after they came back from the laundry. Nurses upstairs were immediately unfolding them and laying them flat. Nobody had asked.
Overprocessing is doing work that provides no value to the patient — entering data into systems nobody reads, clicking through excessive EMR warnings, running centrifuges longer than the manufacturer recommends out of habit. It often results from miscommunications in the handoffs between people or departments. In a billing department, one employee removed “extra” copies from patient charts to save storage space while the next employee in the process walked to the copier to recreate them.
Wasted Human Potential
At one hospital, a nurse said the initial Lean work was “the first time in six years that anybody has asked me what I think about anything.”
This eighth type of waste — sometimes called the waste of talent — is what happens when organizations fail to engage people’s minds. It includes skilled professionals doing work below their training level: nurses doing tasks that could be handled by nursing assistants, pharmacists doing work that pharmacy techs could do. It also includes the subtler loss that occurs when employees stop offering ideas because they’ve learned nobody is listening. One laboratory technologist with more than 25 years of experience said, “Nowadays, I feel like a robot.” Managers had rarely asked for opinions or ideas. Through Lean, employees can have their intelligence and creativity put to use, even when the hands-on work itself has become highly automated.
Final Thoughts
The eight wastes are more than abstract categories–they’re the everyday frustrations that get in the way of providing the care we aspire to deliver. When we learn to see waste clearly, we also learn to see possibilities: more time with patients, fewer interruptions, safer care, and less stress on the people doing the work. The examples from Virginia Mason, the NHS, and TCAB show what becomes possible when organizations treat waste as a solvable problem rather than an inevitable reality.
But identifying waste requires something deeper than training: it requires psychological safety. Waste hides in plain sight when people have learned that speaking up leads to blame. Eliminating waste isn’t about asking people to work harder — it’s about redesigning systems so people can do their best work without constantly battling obstacles. That begins when leaders model curiosity, ask questions instead of giving answers, and respond to problems with appreciation rather than frustration.
Lean gives us a shared language and a practical framework, but the real work happens in conversations, experiments, and small steps forward. If we focus on learning rather than blaming, and on systems rather than heroics, we free up time and capacity for what matters most: caring for patients and supporting the people who care for them.
As always, continuous improvement is a journey. Seeing waste is the first step; creating the psychological safety to discuss it–and to try something new–is how meaningful, sustainable change takes hold.
Frequently Asked Questions
What are the eight types of waste in healthcare?
The eight types of waste are defects, overproduction, transportation, waiting, inventory, motion, overprocessing, and non-utilized talent. The first seven come from Taiichi Ohno’s original framework at Toyota. The eighth — wasting people’s talent and ideas — was added later and matters enormously in healthcare, where the people are the product.
What is the most common type of waste in hospitals?
Waiting is probably the most visible. Patients wait for appointments, test results, discharge paperwork, and the next step in their care. But the waste of motion may be the most pervasive — nurses in many hospitals spend only about 30% of their time on direct patient care because of walking, searching for supplies, and navigating workarounds.
What is an example of overproduction waste in healthcare?
Ordering diagnostic tests that aren’t medically necessary is a common example. So is preparing medications that go unused when a patient’s orders change or they’re discharged before the medication is administered.
What is the waste of non-utilized talent in healthcare?
It’s what happens when skilled people spend their time on work below their training level — nurses doing tasks that could be handled by nursing assistants, pharmacists doing work that pharmacy techs could do. It also includes the waste of not asking employees for their ideas. At one hospital, a nurse said the initial Lean work was “the first time in six years that anybody has asked me what I think about anything.”
How can hospitals reduce waste without cutting corners on patient care?
Lean methods focus on eliminating wasteful steps so people can spend more time on the work that actually helps patients. Virginia Mason Medical Center used Lean to increase nursing time at the bedside from about 33% to 90%. The goal is freeing up time, not cutting resources.
What does DOWNTIME stand for in Lean?
DOWNTIME is a common acronym for the eight wastes: Defects, Overproduction, Waiting, Non-utilized talent, Transportation, Inventory, Motion, and Extra-processing. It’s how most Lean practitioners memorize the list.
How do you identify waste in a hospital?
The most effective method is a gemba walk — going to where the work happens and observing it directly. Many hospitals also use process mapping, time studies, and structured interviews with frontline staff. The eight categories give teams a shared vocabulary for what they’re seeing.



