

Thanks to the organizing sponsor Protegra and other sponsors, including my friends at LeanKit, for having me give a keynote talk about the Software Development and Evolution Conference (SDEC) 2013 Conference in Winnipeg yesterday (Storify summary here).
I always enjoy being around a group of developers (it dredges up memories of my childhood coding on a TI 99/4A computer with a cassette tape storage drive), especially when they are talking about new ways of managing and trying to create a better workplace.
I asked the audience, tongue in cheek, at the start if I was at the wrong conference for two reasons — 1) I was talking about healthcare and 2) I'm an American… but I think there was agreement that the general Lean management principles are applicable across our different domains.
I talked a bit about the sad case of Brian Sinclair, a patient who died in the emergency waiting room after waiting 34 hours without being triaged back in 2008 (the inquiry has been big news in Canada recently).
Some of the elements of the tragedy that speak to fixing the system instead of blaming “bad apples” include:
- Some 17 different staff members saw him in the waiting room, but there wasn't a clear system to indicate that he hadn't been triaged yet
- The E.R. was understaffed by five nurses that day
- It was described by staff as a “war zone” because it was so busy (the data show the patient volume was 10% higher than a normal workday… a properly robust system would be able to absorb that demand variation… but not if they're understaffed)
- There was very poor visibility from the triage station to the waiting aea
- Nobody was fired after the incident (which I think is a positive… the focus should be on fixing the system to prevent future incidents like this)
Again, it's a “bad systems” problem, not a “bad apple” problem.
I shared data about the number of patients who die as the result of adverse events in the U.S. and Canada each year:
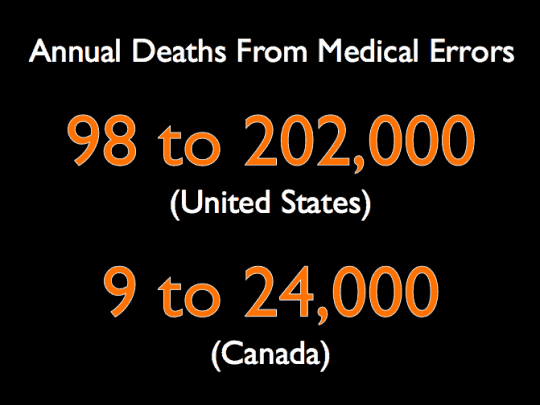
There are wide ranges because it's nearly impossible to accurate count the number of patients who die due to medical errors because of judgment calls and underreporting.
Since Canada's population is about 1/10th that of the U.S. the per-capita harm rates are about the same:
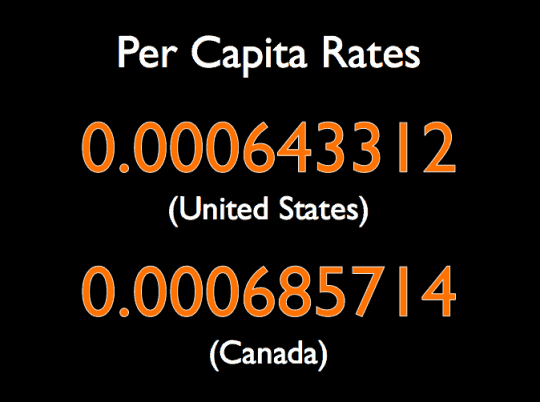
This makes medical harm the THIRD leading cause of death in both countries (after heart disease and cancer). This isn't an American problem or a Canadian problem… it's a global problem.
Even though the U.S. spends twice as much on healthcare as Canada, Canada has longer life expectancy and lower infant mortality. Another global problem is that no country is happy with their current level of healthcare spending or the rate of increase… budgets are stretched and healthcare is now HALF of Canada's government spending.
Even though we have different payer models, the good news is that we CAN learn from each other, across borders (and across industries) about the operational challenges and the system problems that can be fixed with Lean management, Lean thinking, and Lean methods.
My summary of five things we can do to make hospitals better:
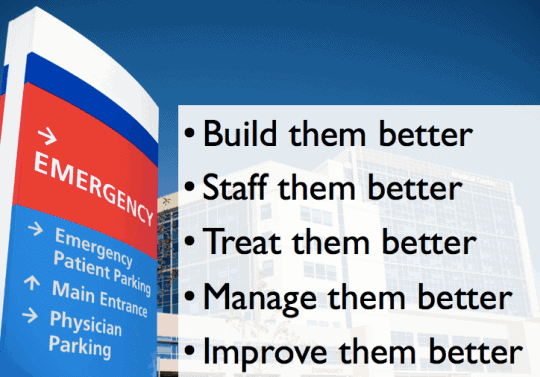
Build them better: Hospitals need to focus on more than just building them prettier. I talked about “Lean Design” efforts at hospitals like Seattle Children's Hospital and the Children's Hospital of Saskatchewan (video). A hospital built with Lean methods engages staff (and patients!!) in the process early on and uses an iterative design process and prototypes to make sure the space properly supports the staff, the right process, and the patients – and gets built better, faster, and cheaper than traditional methods.
Staff them better: I talked about the need to use data to staff a hospital properly, such as looking at patient arrival patterns to the Emergency Department (which are actually quite predictable) and not just staffing “the way it's always been done.”
Treat them better: Hospitals need to not just provide good service to patients (smiles, good food, TV, etc.) but they need to improve the way they treat patients from a clinical perspective – using Lean methods to reduce “door to balloon” times and to reduce infections. Again, the problem is bad systems, not bad people.
Manage them better: Leaders need to go to the “gemba” where work is actually done and then NOT blame people for problems. We need to support the people doing the work to make it easier for them to do the right things the right way.
Improve them better: Shift from top down command-and-control thinking to a Kaizen approach that engages everybody in improvement every day.
It was great talking with people about the parallels to the Lean software, Agile, and Lean Startup worlds:
- People shouldn't hate coming to work
- We assume people want to do quality work and management systems need to allow this
- Shifting away from command-and-control thinking
- Being extremely customer focused and providing a solution, not just tools or code
- Use iterative design principles to test software, websites, buildings, or processes
Thanks again for the chance to visit Winnipeg!
I also had the opportunity to spend a few hours with my friends at St. Boniface General Hospital, a member of the Healthcare Value Network. I met with people from their Transformation department, along with the CEO and CMO who have been VERY engaged in actively leading their Lean journey, which is now five years old.
Check out their website about their Transformation work and this 2010 article from the Winnipeg paper (and my blog post about it).
As ThedaCare, Virginia Mason Medical Center, and others practice, St. Boniface had BOTH a “Rapid Improvement Event” taking place AND daily continuous improvement methods being used in parallel. That's always great to see, as opposed to relying ONLY on the weeklong events.
What do you think? Please scroll down (or click) to post a comment. Or please share the post with your thoughts on LinkedIn – and follow me or connect with me there.
Did you like this post? Make sure you don't miss a post or podcast — Subscribe to get notified about posts via email daily or weekly.
Check out my latest book, The Mistakes That Make Us: Cultivating a Culture of Learning and Innovation:







{kind=link}
Excellent post, Mark. Some good advice for lean healthcare professionals, and all healthcare professionals for that matter.
Great post Mark, just like past ones.Wondering if you had any experience or worked on interesting projects on the health insurance side of the business.
Thanks, Sunny… no, I have not ever worked on the insurance side of things…