

So I'm finally watching the DVR-ed episode from March 10, 2009 that gave widespread exposure to the issue of medical mistakes. Oprah began the show by citing the statistic that errors cause more deaths than “breast cancer, AIDS, and car accidents combined.” This is not hyperbole.

Dr. Oz was on to talk about this issue for the first time on Oprah's show (where has he been on this?). Yes, 100,000 lives per year.
Dennis Quaid and his wife Kimberly appeared on the show discussing the incident that could have killed his newborn twins, something I've blogged about here (and see some video from Oprah here).
They recounted the story of how the twins were mistakenly given adult doses of blood thinner (10,000 times the dose they needed) TWICE. Not once, but on two separate occasions. The original focus in the story was “a nurse” gave the wrong doses… it's not fair to pin the blame only on the nurse who administered the dose. What in the system allowed this wrong mediation to even get that far?
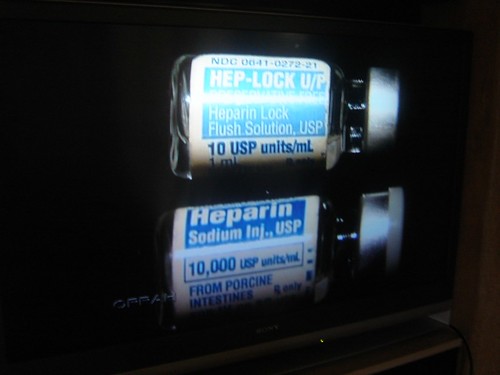
Look at the vials with different doses as used then at Cedars Sinai. See how similar the blues look, especially given that they're the same size and they might be seen in a dark room at 2 am.

The hospital was, unfortunately, using the OLD inventory (the similar blues) rather than using the NEW inventory from the vendor that had better error proofing because of different colors and different methods for opening the vial. The hospital chose saving some money (not just throwing away or donating the old stock) over preventing the problem. See the 2nd picture for the new packaging — see how much harder it would be to make a mistake?
People knew about the look-alike packaging problem in 2006. Why didn't Cedars Sinai take more preventative action before this problem occurred in late 2008?
Early in the show, Dennis was talking about his lack of vigilance, that he expected that hospitals take care of you, that things will be OK, and that “people know what they're doing… but mistakes happen.”
In situations like this, the people “know” what they're supposed to do (give the right dose), but errors occur due to systemic failures and bad processes.
In talking about the incident, Dennis said that maybe it happened for a reason, that this can increase awareness and help get this problem solved. Amen to that. Any episode like this should drive process improvement and error-proofing work at Cedars Sinai and every hospital.
Dennis suggested “computerized record keeping and bar code scanning” as a solution, which probably shows our American bias toward technology solutions. Dr. Oz pointed out (correctly) that we use a 19th-century tool (a pen) in a 21st-century medical system. He states that these technology solutions do help. But would they prevent EVERY incident? Not if nurses are clever enough to find ways to work around the bar coding systems when they are overwhelmed and pressed for time. This is a management/process problem, not just a technology problem. It's naive to think that technology alone can solve this problem.
Quaid returned to Cedars-Sinai, with the Oprah cameras, and met with the Chief Nursing Officer, who said the overdose incident was “life-changing” for her and her nurses, that “there was a lot of crying, a lot of hand-wrenching.” OK, that proves that people care, nobody doubts that. Nobody WANTS to make an error like this, but the systems failed the nurses.
Crying and feeling bad isn't enough when they could have been more proactive to improve their systems, learning from the Indianapolis case and other previous incidents. Where was the hand wringing when they realized this COULD happen at Cedar Sinai? Did they read the news about the Indianapolis case from 2006 and think “well we're better, it couldn't happen here”?
The CNO said this incident “served as a catalyst to find ways to prevent these errors.” That's good.
The timeline that actually occurred:
- 2006: Heparin overdose kills 3 babies in Indianapolis
- 2008: Heparin overdose severely harms the Quaid twins
- 2008: Cedars Sinai staff feel bad and begin improvement
- 2009: Oprah episode
It's too bad the timeline wasn't this:
- 2006: Heparin overdose kills 3 babies in Indianapolis
- 2006: Cedars Sinai staff recognize systemic risk and improve their processes
- 2008: Quaid twins are not overdosed
- 2009: No Oprah episode
How did the incident occur?
- Pharmacy tech made an error and put large dose Heparin in the same bin as small doses (see picture).
- The nurse grabbed a bottle out of the bin without checking the label (Quaid pointed out that the colors of the bottles are very similar, so they're hard to tell apart)
Since the incident, Cedars Sinai has implemented a bar code system (as pictured). Their medical cabinets (commonly found in hospitals, this is not cutting edge technology) will “only dispense the dose that's been ordered). But what if someone mis-loads the cabinet?
Quaid said “if this system had been in place when our kids were here, I don't think this could have occurred.” There are still holes in these systems, the technology isn't perfect error proofing because we still rely on people properly following processes. There's still a risk that staff cut corners and managers need to be aware of that possibility. Managers need to audit the process and make sure workarounds aren't being employed, communicating consistently about how important it is to follow the process. Then, the managers have to make sure that people have time to do things the right way (by having correct staffing levels and by eliminating waste in the process so nurses don't fall behind in their work because they're running around searching for tools and equipment).

During their demonstration, Quaid and Oprah inadvertently nearly showed one of the workarounds — scanning an extra bar code label that was NOT on a patient's arm. He was struggling to put the bar code on Oprah, so Quaid pulled the label toward Dr. Oz. (click any picture for a larger version)

To the credit of Dr. Oz, he prompted Quaid to properly demonstrate it by sort of putting the wrist band around Oprah's wrist. Dr. Oz demonstrated the signal that would be given by the technology if he tried scanning a med for which no order appeared, a med that could have made her collapse.
Dr. Oz states that hospitals that have implemented systems like the one he demonstrated have gotten errors of the type that harmed the Quaid twins down to ZERO.
After the demo, Quaid also correctly pointed out some of the human factors:
- Nurses who are working 24-hour shifts
- They have a lot of patients
So errors occur. “Human error is part of the process,” said Quaid, so systems like this bring down the number of episodes. But will it really become ZERO if we don't have good process controls and error proofing?
I wish there had been more focus in the discussion about process and management, not just technology. I will applaud Quaid and Oprah (and Dr. Oz) for trying to increase awareness. Now we just need the right countermeasures and a full set of process and technology countermeasures, both.
What do you think? Please scroll down (or click) to post a comment. Or please share the post with your thoughts on LinkedIn – and follow me or connect with me there.
Did you like this post? Make sure you don't miss a post or podcast — Subscribe to get notified about posts via email daily or weekly.
Check out my latest book, The Mistakes That Make Us: Cultivating a Culture of Learning and Innovation:







{kind=link}
Talk’s cheap…how are the twins?
The twins have recovered and will lead normal lives.
Does that excuse their mistakes?
Not sure what you’re getting at with the “talk is cheap” comment.
Mark:
Not at all. There is no excuse for anyone in any segment of the medical field losing site of the ultimate customer – the patient – and the family members.
I recently did some work in a “Baldrige Award Winning” hospital. (That’s what their P/R campaign calls them.) The callous treatment of patients and their families in favor of slaving to the charts, checklists, computers and process reminders was so obvious that I once counted 7 family members standing in the doorways of their respective patients’ rooms looking expectantly toward the nurses’ station. (There were only 9 rooms on that end of the hall.)
The conversations I later gathered from those families was not flattering. Taken literally, some of the comments were outright frightening.
My comment about “talk is cheap” simply refers to the endless debates about “the how” of continual improvement initiatives. So many efforts fail because the customer gets lost in the rhetoric, demonstrations, meetings, metrics, tools, terms, techniques, etc.
None of these initiatives or methods are inherently bad. Rather, the execution – apart from current customer requirements – simply fails to make the improvements that customers want.
Love the blog.
Anon — well put!
First, you have to have the right focus (patient — safety and quality being primary).
Second, you have to WANT to change (and not just make excuses).
Third, you have to set the bar HIGH, aim for perfection, not just beating benchmarks.
Fourth, you have to be PERSISTENT to fight through difficulties that will come up with trying to change.
Many organizations (including hospitals) who say “we are doing Lean” (or any other such method) are not meeting the test of the first four points above and they’re probably wasting their time.
You’re right, it’s not just “by what method” but “why” that’s required.
As Dr. Deming always said… survival is not mandatory.
[…] (ratings?) while the crisis of preventable medical errors gets so little attention unless a celebrity’s babies are harmed? So I made this graphic. Please feel free to share via social […]
[…] of preventable mistakes that killed three babies in an Indianapolis hospital in 2006, leading to the 2009 overdose of the Quaid twins (which they survived, […]
[…] don’t post warning signs that say, “Caution: Don’t give the babies the wrong medication” or “Warning! Don’t mix up the laboratory specimens.” I’m glad they don’t have signs […]
[…] desiring). Far too often, I see news reports where something bad happens in a hospital (like the Quaid twins getting the wrong medication) and a C-level executive says “Procedures were not followed and there’s no excuse for […]
[…] Dennis Quaid and Medical Mistakes Episode on Oprah […]
[…] My Notes on the ‘Oprah’ Epsiode with Dennis Quaid About Medical Mistakes […]